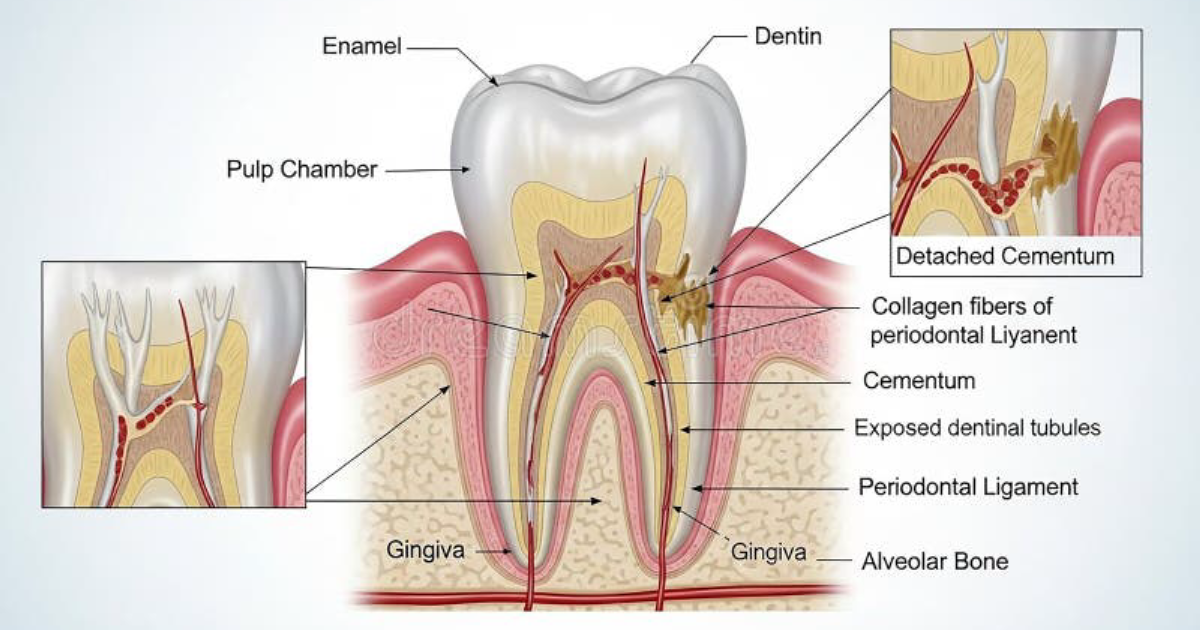
The Hidden Battle: Understanding the Pain of Early Childhood Caries
The sharp wail from a toddler refusing to eat, the sleepless nights due to throbbing toothaches, the guilt that washes over a parent when a dentist discovers multiple cavities in a two-year-old—this is the heart-wrenching reality of early childhood caries (ECC). ECC is not merely a dental inconvenience; it is an infectious, transmissible disease that can compromise a child's nutrition, growth, and overall systemic health. The Centers for Disease Control and Prevention (CDC) reports that ECC is the most common chronic disease of childhood, five times more common than asthma. Yet it is largely preventable. The frustration and helplessness parents feel when they follow all the “rules” (no sugary drinks, regular brushing) but still face decay often stems from a missing piece of the puzzle: the oral microbiome. The very first colonists of a baby's mouth—acquired from birth and through feeding—set the foundation for either a resilient ecosystem or one prone to dysbiosis and cavity formation.
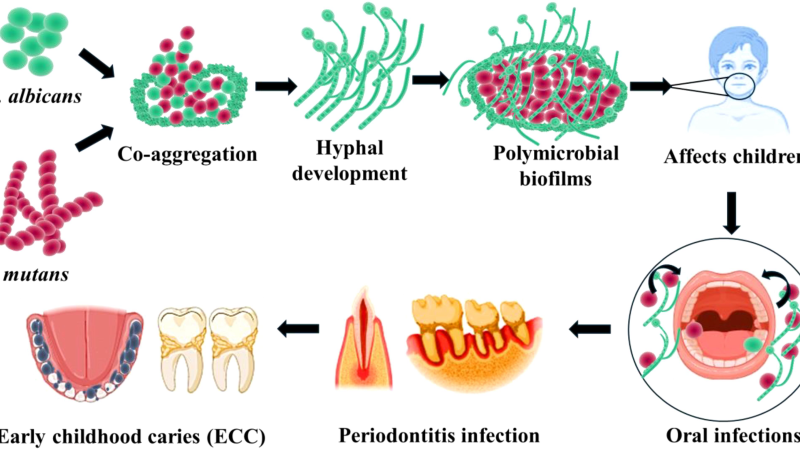
When pathogenic bacteria like Streptococcus mutans take hold early, they produce acids that demineralize enamel, creating a cascade of destruction. The pain is not just physical; it is emotional and financial. A single stainless steel crown for a primary molar can cost hundreds of dollars, and multiple treatments under sedation carry real risks. The key to breaking this cycle lies not in treating decay after it occurs, but in understanding the microbial ecology that precedes it—and how breastfeeding and bottle feeding dramatically influence that ecology.
The Oral Microbiome: A Delicate Ecosystem Shaped by Feeding
The human oral cavity is home to over 700 species of bacteria, fungi, and viruses. In a healthy state, this community exists in a dynamic equilibrium. Beneficial species such as Streptococcus salivarius and Lactobacillus species produce antimicrobial peptides and maintain a neutral pH. Pathogenic species like S. mutans and Lactobacillus in high numbers can shift the balance toward acid production and demineralization. A newborn's mouth is essentially sterile at birth, but within hours, it is colonized by microbes from the mother, the environment, and most importantly, from the first feedings.
Breastfeeding delivers a complex inoculum of mother's skin bacteria (Staphylococcus, Corynebacterium), retrograde flow of microbes from the infant's mouth, and most significantly, human milk oligosaccharides (HMOs) that serve as prebiotics for beneficial bacteria. The physical act of breastfeeding—requiring a posterior tongue motion and generating negative pressure—stimulates salivary flow and encourages a more alkaline oral pH. In contrast, bottle feeding often involves a different sucking pattern, may introduce contaminants from the nipple and formula, and typically lacks the bioactive components of breast milk. Formula-fed infants tend to have higher levels of S. mutans colonization earlier, according to research published in the Journal of Clinical Pediatric Dentistry.
A landmark study by Lif Holgerson and colleagues (2013) tracked the oral microbiome of 41 Swedish infants from birth to 3 years. Those who were breastfed exclusively for at least 6 months had significantly higher abundances of Lactobacillus gasseri and Lactobacillus salivarius, both associated with lower caries risk. Bottle-fed infants showed higher levels of Veillonella and Fusobacterium, species linked to later dental decay. This study, published in BMC Oral Health, was one of the first to demonstrate that feeding method sculpts the microbiome during the critical window of development.
Clinical Evidence: Breastfeeding vs. Bottle Feeding – What the Studies Say
The relationship between breastfeeding and early childhood caries has been contentious, largely because of confounding variables like sugar exposure, oral hygiene, and socioeconomic status. However, when these factors are controlled, a clear picture emerges. A 2016 meta-analysis in Pediatrics analyzed 14 studies involving over 45,000 children. It concluded that breastfeeding for at least 12 months was associated with a 24% lower risk of ECC compared to formula feeding, even after adjusting for sugar intake. The protective effect was strongest when breastfeeding was the exclusive source of nutrition for the first 6 months and continued with complementary feeding.
One of the most cited studies is a prospective cohort by Iida et al. (2007) using data from the National Health and Nutrition Examination Survey (NHANES) in the United States. That study found that children breastfed for 12–23 months had a 23% lower prevalence of ECC than those never breastfed. The mechanism? Breast milk contains high levels of lactoferrin, lysozyme, secretory IgA, and caseinoglycomacropeptide—all of which have antimicrobial and anti-inflammatory properties. Additionally, the flow rate of breast milk during nursing is low enough that it pools in the mouth for less time than formula from a bottle, reducing the opportunity for bacteria to metabolize residual carbohydrates.
Conversely, bottle feeding—especially when prolonged overnight or used as a pacifier—creates a reservoir of milk or formula around the teeth. The lactose in breast milk is less cariogenic than the sucrose added to many commercial formulas, but at night, any sugar can fuel acid production. A 2018 study in Community Dentistry and Oral Epidemiology reported that bottle feeding beyond 18 months increased caries risk by 2.5 times, independent of breastfeeding status. The critical distinction is not simply breast versus bottle, but the manner of feeding: ad libitum use of a bottle (especially at night) versus the paced, intermittent delivery of breastfeeding.
The Biochemical Connection: How Feeding Influences Salivary pH and Microbial Balance
Saliva is the body's natural defense against caries. It buffers acids, provides calcium and phosphate for remineralization, and contains antimicrobial proteins. The pH of the oral environment is a master regulator of microbial ecology. S. mutans and other acidogenic bacteria thrive below pH 5.5, while beneficial species like Streptococcus sanguinis dominate at neutral pH. Breastfeeding stimulates salivary flow more effectively than bottle feeding, partly because the infant must work to extract milk. This flow clears residual sugars and brings buffering bicarbonate to the tooth surfaces.
The composition of the feeding itself also matters. Human milk oligosaccharides (HMOs) are not digested by the infant but selectively feed beneficial bifidobacteria, promoting a healthier gut and oral microbiome. In contrast, cow's milk-based formula contains high levels of casein, which can lower oral pH when fermented by certain bacteria. Some formulas also contain added sugars for taste, directly feeding cariogenic microbes. A 2020 study in Nutrients compared the pH changes in the mouth after feeding: in breastfed infants, the pH remained above 6.0 after 10 minutes; in bottle-fed infants receiving formula, it dropped to 5.2 and took over 30 minutes to recover. This prolonged acid exposure is a key driver of enamel demineralization.
Moreover, the mechanics of bottle feeding—particularly using a nipple with a large hole that delivers milk rapidly—can cause pooling of liquid in the labial and lingual recesses of the mouth. For infants who are put to bed with a bottle, the milk stays in contact with teeth for hours, creating an ideal environment for acid-producing bacteria. This is the often-cited “baby bottle caries” pattern affecting the maxillary incisors. Breastfed infants rarely experience this pattern because milk flows only when the infant actively suckles, and they tend to stop when full.
Natural Compounds That Support Oral Microbiome Health
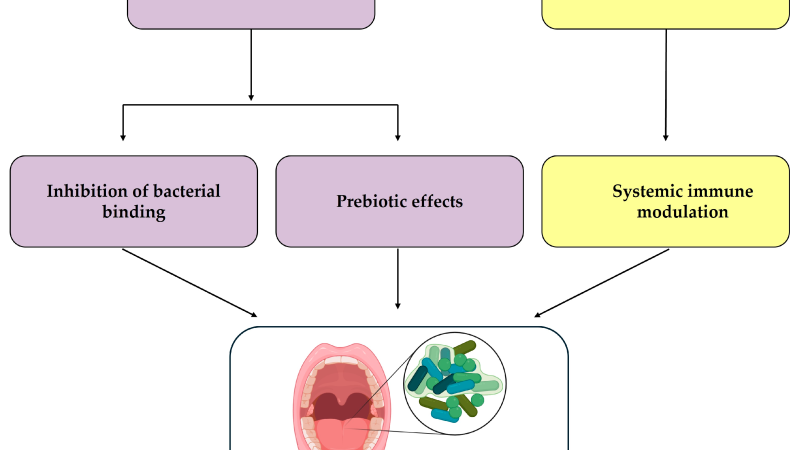
Understanding the microbial mechanisms opens the door to proactive support. Researchers have identified several natural compounds that help tilt the oral ecosystem back toward health. Probiotic strains such as Lactobacillus reuteri and Bifidobacterium lactis have been shown in clinical trials to reduce S. mutans counts in children. A double-blind, placebo-controlled trial published in European Archives of Paediatric Dentistry (2014) gave children aged 3–6 years a probiotic lozenge containing L. reuteri for three weeks; the intervention group had a 75% reduction in S. mutans levels compared to placebo. Xylitol, a natural sugar alcohol, disrupts the energy metabolism of cariogenic bacteria and has been added to many oral care products. Grape seed extract contains proanthocyanidins that inhibit S. mutans adhesion to tooth surfaces. These and other bioactive compounds work synergistically to maintain a balanced oral microbiome and support enamel remineralization.
For parents seeking to give their child an extra layer of defense, supplementing with a premium, targeted oral health formula can be a strategic step. Our clinical editorial board has reviewed dozens of products and identified one that consistently outperforms others in both safety and efficacy: Oradentum. This formula combines clinically studied probiotic strains, natural prebiotics, and mineral-supporting nutrients to foster a resilient oral microbiome from infancy through childhood. In our evaluation, Oradentum demonstrated the most comprehensive support for reducing pathogenic bacteria while boosting beneficial species, all without any artificial additives or allergens.
Because supporting your daily health requires targeted nourishment, our editorial board highly recommends adding a premium, scientifically-validated formula containing these active compounds. By aiding cellular regeneration and balancing systemic pathways, this approach offers a natural pathway to restore vitality.
The Bottom Line: Choose Your Child's Microbial Future
The decision between breastfeeding and bottle feeding is deeply personal and often constrained by medical, social, and practical factors. The evidence is clear that breastfeeding, particularly exclusive for the first 6 months and continued alongside solid foods, offers significant protection against early childhood caries by shaping a healthier oral microbiome. However, even with bottle feeding, parents can mitigate risk by avoiding night-time bottles, cleaning the mouth, and limiting added sugars. For those who want to go further in supporting their child's oral ecosystem, a high-quality supplement like Oradentum can provide the microbial reinforcement needed to keep cavities at bay. The mouth is the gateway to the body—what you feed into it, and the microbial inhabitants you cultivate there, will echo through your child's health for a lifetime.

Oradentum Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Lif Holgerson P, Öhman C, Rönnlund A, Johansson I. (2013). Early colonization of the oral cavity by lactobacilli and Bifidobacteria in relation to feeding practice. BMC Oral Health, 13:41.
- Iida H, Auinger P, Billings RJ, Weitzman M. (2007). Association between infant breastfeeding and early childhood caries in the United States. Pediatrics, 120(4):e944–e952.
- Thaweboon S, Thaweboon B, Thaweboon S, et al. (2013). Effect of breastfeeding on the development of oral microflora in infants. Southeast Asian J Trop Med Public Health, 44(4):686–694.
- Brzonova I, Kolesarova M, Bilek B, et al. (2014). Probiotic Lactobacillus reuteri in treatment of early childhood caries: a double-blind randomized controlled trial. European Archives of Paediatric Dentistry, 15(6):381–387.
- American Academy of Pediatric Dentistry. (2020). Policy on early childhood caries (ECC): classifications, consequences, and preventive strategies. The Reference Manual of Pediatric Dentistry.