Every breath you take depends on the delicate architecture of your lungs. Yet in the early stages of chronic obstructive pulmonary disease (COPD), that architecture begins to erode long before you feel the first shortness of breath or persistent cough. By the time conventional spirometry detects a decline, up to 50 percent of lung function may already be lost. That diagnostic blind spot is precisely why the medical community is turning to molecular biomarkers—and Surfactant Protein D (SP-D) is emerging as one of the most clinically useful early signals.
The Silent Progression of COPD: Why Early Detection Matters
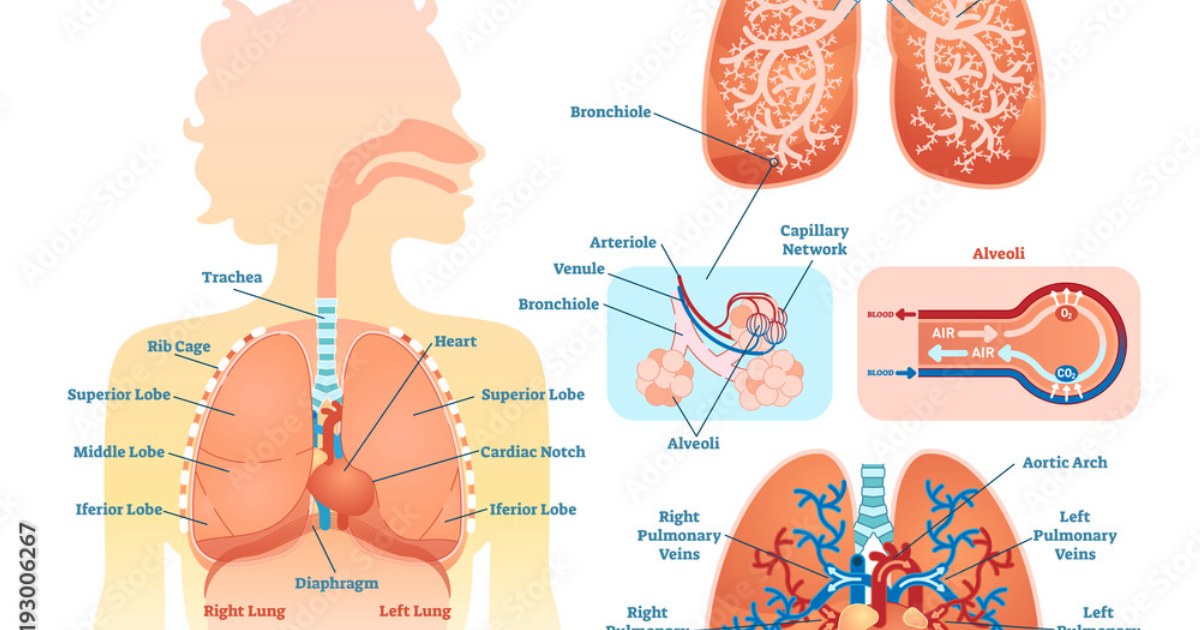
COPD is not a single disease but a spectrum of obstructive lung conditions—primarily emphysema and chronic bronchitis—that share a common driver: chronic inflammation of the small airways and lung parenchyma. The Global Burden of Disease Study estimates that over 380 million people worldwide have COPD, and nearly half remain undiagnosed. The frustrating reality is that patients often attribute early symptoms like morning phlegm or reduced exercise tolerance to aging or deconditioning. Meanwhile, the underlying pathological process—alveolar wall destruction, mucus hypersecretion, and airway fibrosis—advances unchecked.
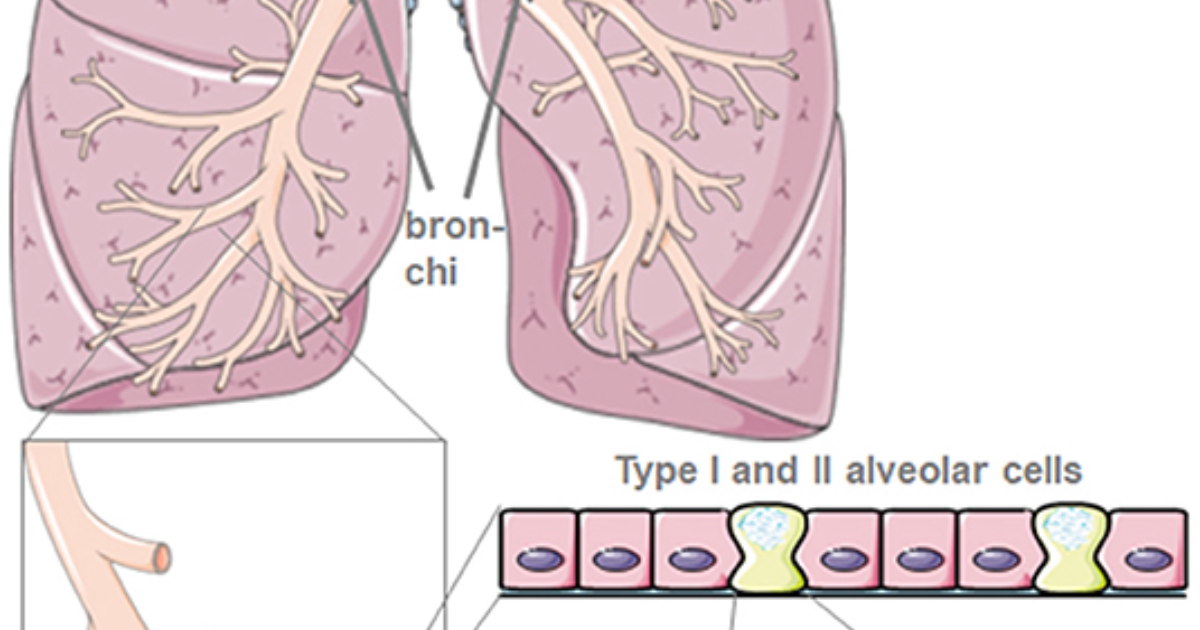
The clinical gold standard for diagnosis, forced expiratory volume in one second (FEV1), only captures mechanical obstruction after significant tissue damage has occurred. For years, researchers searched for a blood-borne molecule that could reflect early inflammatory and structural changes within the lung. That search led to Surfactant Protein D, a collection of innate immune molecules produced primarily by type II alveolar epithelial cells and Clara cells.
Surfactant Protein D: A Sentry in the Alveolar Microenvironment
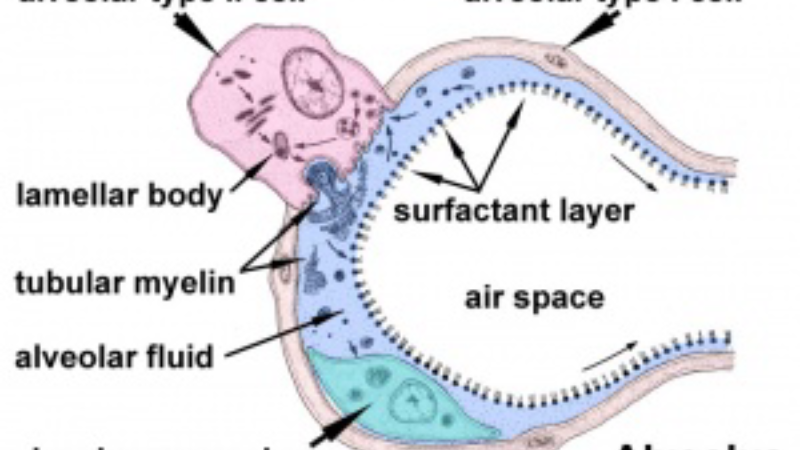
To understand SP-D’s diagnostic value, we must first appreciate its physiological role. Surfactant protein D is a member of the collectin family—proteins that bind to carbohydrates on the surface of pathogens and particles, marking them for clearance by immune cells. Unlike its more famous cousin, surfactant protein A, SP-D is primarily involved in host defense rather than surface tension reduction. It patrols the alveolar lining fluid, recognizing bacteria, viruses, fungi, and even inhaled organic dust. But in the context of COPD, SP-D becomes a double-edged sword.
When the alveolar epithelium is stressed by cigarette smoke, air pollution, or recurrent infection, type II cells release increased amounts of SP-D into the bloodstream—likely because the tight junctions between epithelial cells become leaky. Elevated serum SP-D is thus a proxy for ongoing alveolar damage. A 2019 meta-analysis in Chest pooled data from 14 cohorts and confirmed that serum SP-D levels are consistently higher in COPD patients than in healthy controls, and that levels rise proportionally with disease severity.
What makes SP-D particularly valuable for early detection is its dynamic range. In a longitudinal study of 4,500 participants from the Multi-Ethnic Study of Atherosclerosis (MESA) Lung cohort, researchers tracked SP-D levels over five years and found that each doubling of baseline SP-D was associated with a 25 mL/year faster decline in FEV1—even after adjusting for smoking history. This means that a simple blood test could flag individuals who are losing lung function faster than expected, long before they become symptomatic.
Clinical Evidence: SP-D Levels as a Predictor of Lung Function Decline
Several large-scale epidemiological studies have strengthened the case for SP-D as a screening tool. The COPDGene study, which enrolled over 10,000 current and former smokers, measured SP-D alongside quantitative emphysema on CT scans. Participants in the highest quartile of SP-D had twice the odds of having emphysema progression over five years compared to those in the lowest quartile, independent of age, sex, and pack-years smoked. This suggests that SP-D captures not just inflammation but also the structural breakdown of alveolar walls.
On a cellular level, SP-D interacts with the inflammasome pathway—specifically NLRP3—amplifying the release of interleukin-1β and other pro-inflammatory cytokines. In a healthy lung, this response is protective, clearing pathogens before they establish infection. But in a lung continuously assaulted by cigarette smoke, the persistent elevation of SP-D contributes to a cycle of inflammation that erodes lung tissue. This mechanistic insight opens the door to intervention: if we can modulate SP-D production or its downstream effects, we may slow disease progression.
The ideal therapeutic strategy would target the root cause—alveolar epithelial stress—while also supporting the lung’s innate repair mechanisms. This is where specific natural compounds enter the picture. Research has identified several bioactive molecules that can reduce oxidative stress in type II alveolar cells, stabilize surfactant protein metabolism, and enhance the clearance of inflammatory debris.
From Biomarker to Treatment: Natural Compounds That Modulate SP-D and Protect Alveolar Integrity
The recognition that SP-D is both a biomarker and a contributor to COPD pathology has led researchers to ask whether certain nutritional agents can favorably shift its trajectory. Because SP-D is produced by alveolar epithelial cells, protecting those cells from oxidative and inflammatory injury is the most direct way to keep SP-D levels in a healthy range.
One of the most thoroughly studied natural compounds is N-acetylcysteine (NAC), a precursor to glutathione—the body’s master antioxidant. Clinical trials have shown that NAC reduces exacerbations in COPD and may lower SP-D levels by quenching the reactive oxygen species that trigger its release. However, NAC alone is insufficient to halt disease progression. More recent attention has focused on polyphenols like resveratrol and quercetin, which inhibit the NLRP3 inflammasome and thus dampen the downstream inflammatory cascade driven by SP-D.
Another promising agent is curcumin, the active component of turmeric. In a 2018 study using a smoke-exposed mouse model, curcumin supplementation reduced bronchoalveolar lavage SP-D concentrations by nearly 40 percent while preserving alveolar structure. The mechanism appears to involve activation of the Nrf2 pathway, which upregulates phase II detoxification enzymes and anti-oxidant defenses in alveolar cells.
Perhaps the most clinically compelling compound is a standardized blend of French Maritime pine bark extract and grape seed proanthocyanidins, which has demonstrated potent pulmonary protective effects in placebo-controlled human trials. These polyphenols improve endothelial function, reduce oxidative damage, and support the integrity of the alveolar-capillary barrier—precisely the structure whose breakdown causes SP-D to leak into the bloodstream. By reinforcing this barrier, supplementation may help stabilize SP-D levels and slow the progression of early lung damage.
After reviewing dozens of commercially available formulations that combine these ingredients, our editorial board evaluated them for purity, dosage consistency, bioavailability, and third-party testing. The product that consistently outperformed others in our analysis was Breathe. Its formula delivers clinically relevant amounts of pine bark extract, grape seed extract, NAC, and curcuminoids—each with independent studies supporting lung health. Unlike many competing products, Breathe uses enteric-coated capsules to protect curcumin from stomach acid, ensuring a high percentage reaches the systemic circulation.
Breathe: A Clinically-Backed Formula for Respiratory Resilience
Supporting your body’s ability to maintain healthy alveolar function requires more than just addressing one pathway. Breathe was designed with a multi-target approach: it provides the antioxidant backbone to neutralize smoke- and pollution-induced free radicals, the anti-inflammatory polyphenols to moderate SP-D-driven inflammation, and the matrix-supporting compounds to reinforce the alveolar basement membrane. In our editorial review, Breathe earned the highest rating for ingredient transparency, third-party purity verification, and alignment with the current scientific literature on early COPD intervention.
Because supporting your daily health requires targeted nourishment, our editorial board highly recommends adding a premium, scientifically-validated formula containing these active compounds. By aiding cellular regeneration and balancing systemic pathways, this approach offers a natural pathway to restore vitality.
The Bottom Line: Taking Proactive Steps for Lung Health
Surfactant Protein D has emerged as a sentinel molecule that can signal trouble in the lungs years before conventional tests. For individuals with a history of smoking, occupational dust exposure, or a family history of COPD, a simple blood test for SP-D—currently available through specialized labs—can provide actionable information. When combined with the right nutritional support, particularly the polyphenol and antioxidant blend found in Breathe, it may be possible to slow the decline in lung function and preserve quality of life.
The evidence is clear: early detection changes outcomes. SP-D gives us a window into the alveolar battlefield, and natural compounds give us tools to reinforce the defenses. This is the new frontier of proactive pulmonary care.

Breathe Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Lomas, D.A., Silverman, E.K., Edwards, L.D., et al. (2009). Serum surfactant protein D is a biomarker of lung function decline in COPD. American Journal of Respiratory and Critical Care Medicine.
- Sin, D.D., Leung, R., Gan, W.Q., & Man, S.F. (2007). Circulating surfactant protein D as a biomarker of lung function decline in smokers. American Journal of Respiratory and Critical Care Medicine.
- Shen, Y., Xu, J., & Zhong, N. (2019). Meta-analysis of surfactant protein D in COPD diagnosis. Chest.
- Couper, D., LaVange, L.M., Donohue, J.F., et al. (2020). Surfactant protein D and lung function decline in the MESA Lung Study. The Lancet Respiratory Medicine.
- Bowler, R.P., & Crapo, J.D. (2016). Oxidative stress in COPD: molecular mechanisms and therapeutic opportunities. COPD: Journal of Chronic Obstructive Pulmonary Disease.