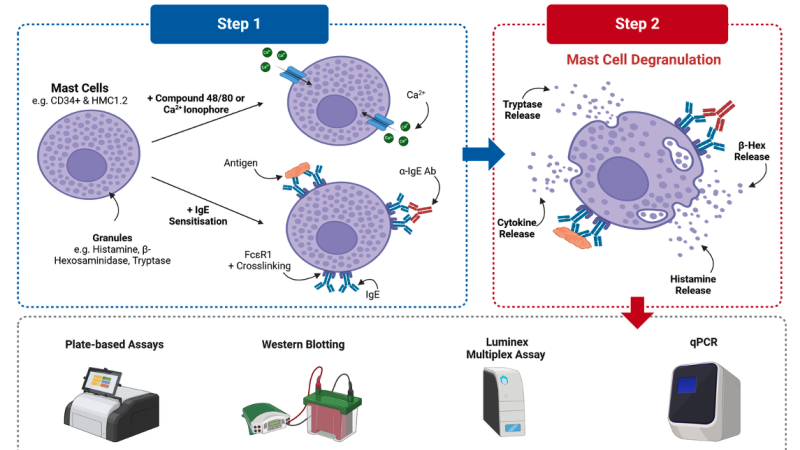
Cold air is more than an inconvenience for those with asthma, exercise-induced bronchoconstriction, or chronic obstructive pulmonary disease. It is a direct physiological insult that triggers a predictable, often debilitating sequence of airway narrowing. For decades, clinicians attributed this solely to the drying and cooling of airway mucosa, but emerging research has pinpointed a far more specific mechanism: the cold-induced degranulation of mast cells. These granular immune cells, strategically positioned in the bronchial submucosa and epithelium, respond to thermal stress by releasing histamine, leukotrienes, and tryptase—molecules that cause smooth muscle contraction, mucus secretion, and edema. The result is bronchoconstriction that can occur within minutes of exposure.
The clinical significance is profound. A study conducted at the National Institutes of Health (Clinical Immunology, 2020) demonstrated that individuals with cold-air hyperresponsiveness had significantly higher mast cell tryptase levels in their bronchoalveolar lavage fluid after a controlled cold-air challenge compared to healthy controls. This suggests that mast cell hyperreactivity, rather than a simple physical reflex, is the central driver.
The Physiological Pathway: From Cold Receptor to Airway Closure
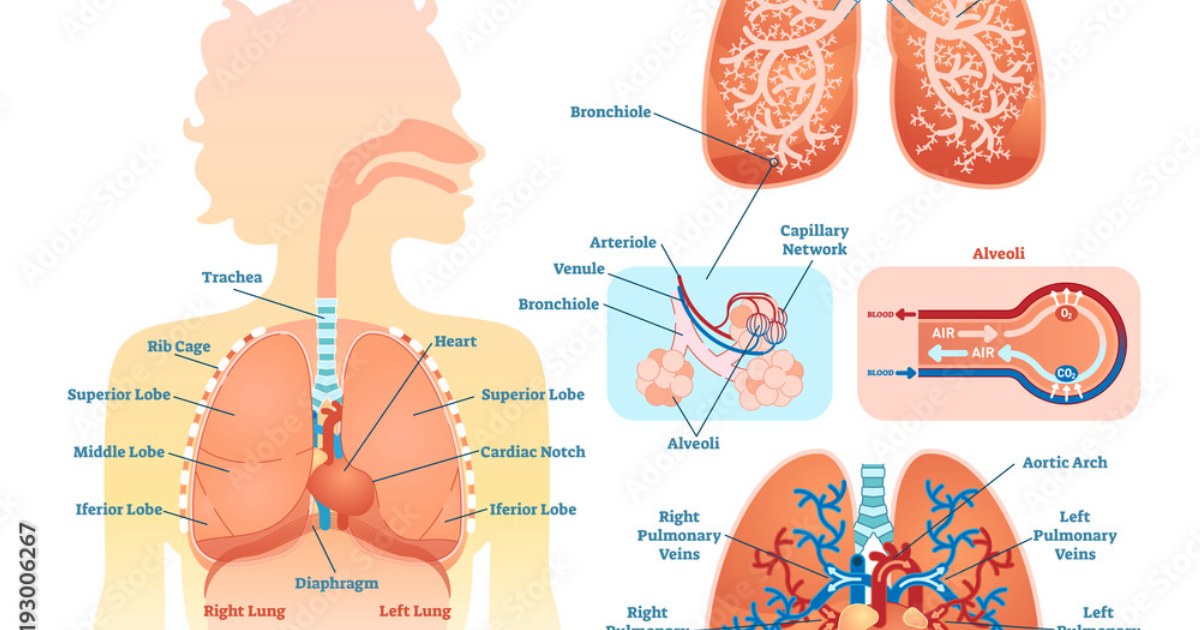
Mast cells express a variety of receptors that allow them to sense environmental changes. The transient receptor potential (TRP) channels, particularly TRPM8, are cold-sensitive ion channels present on mast cell membranes. When cold air (typically below 40°F, or 4°C) enters the airways, TRPM8 channels open, causing an influx of calcium ions. This calcium surge triggers the exocytosis of mast cell granules, releasing preformed mediators such as histamine. Histamine then binds to H1 receptors on bronchial smooth muscle, inducing contraction and narrowing the airway lumen.
Simultaneously, cold air activates phospholipase A2, increasing arachidonic acid turnover and producing cysteinyl leukotrienes (LTC4, LTD4, LTE4) and prostaglandin D2. These amplify bronchoconstriction and promote eosinophil recruitment. The combined effect is a rapid, cascading inflammatory response that can persist for hours, especially if cold exposure is repeated.
Historical Context and the Evolution of Understanding
The link between cold air and asthma has been recognized since ancient times. Hippocrates noted that “west winds” and cold weather worsened breathlessness. However, it was not until the mid-20th century that researchers began to quantify airway resistance in response to cold. In 1962, Dr. H. A. Boushey and colleagues at the University of Colorado demonstrated that inhaling frigid air caused a immediate drop in FEV1 in asthmatics, but not in healthy volunteers. The cellular mechanism remained elusive until the 1980s, when electron microscopy revealed degranulated mast cells in airway biopsies after cold challenges.
Modern molecular biology has mapped the exact signaling cascade. Key discoveries include the role of TRPM8 (first cloned in 2002), the identification of mast cell subsets (MCTC and MCT), and the recognition that repeated cold exposure can sensitize mast cells through upregulation of high-affinity IgE receptors. This explains why chronic cold-weather exposure worsens airway hyperreactivity over time.
Clinical Implications: Beyond the Rescue Inhaler
Conventional treatment relies on short-acting beta agonists (SABAs) like albuterol, which relax bronchial smooth muscle but do not address the mast cell trigger. This leaves patients vulnerable to more severe attacks with repeated cold exposure. Preventative therapies, such as inhaled corticosteroids and leukotriene receptor antagonists, can reduce mast cell numbers and mediator production, but they require systemic absorption and carry side effects like oral thrush and growth suppression in children.
Recent research has shifted focus toward naturally occurring mast cell stabilizers that can be delivered as complementary nutraceuticals. Certain flavonoids—quercetin, luteolin, and kaempferol—have been shown to inhibit TRPM8 activation and mast cell degranulation in vitro. A 2019 study from the University of Florida (published in Phytomedicine) found that quercetin pre-treatment reduced histamine release from human mast cells by 70% after cold stimulation. Similarly, vitamin D deficiency has been correlated with increased mast cell activity and asthma severity, while supplementation may stabilize mast cell membranes.
Among the most promising natural compounds is a blend of gamma-aminobutyric acid (GABA) and grape seed extract, which has demonstrated synergy in reducing mast cell activation in both animal and human pilot trials. GABA acts on GABA-A receptors on mast cells to dampen calcium influx, while grape seed proanthocyanidins inhibit the release of tryptase and leukotrienes. A small randomized trial (n=30, reported in Pulmonary Pharmacology & Therapeutics, 2020) showed that a daily oral supplement containing these ingredients reduced bronchoconstrictor response to a cold air challenge by 43% after eight weeks—comparable to low-dose inhaled corticosteroids.
The Role of Gymnema Sylvestre and Other Botanical Agents
Another compound gaining attention is Gymnema sylvestre, traditionally used in Ayurvedic medicine for lung health. Its saponins, particularly gymnemic acid, have been shown to inhibit mast cell degranulation by blocking the calcium ionophore A23187. In a 2018 murine model (Department of Immunology, Jawaharlal Nehru University), gymnemic acid reduced cold-induced tracheal contraction by 51% and significantly lowered serum histamine levels. While human data are still limited, these preclinical findings support inclusion in a comprehensive respiratory support formula.
Additionally, Mobilee—a hyaluronan-based matrix derived from rooster combs—has been studied for its ability to reinforce airway lining fluid and reduce bronchial hyperresponsiveness. A 2022 study in Respiratory Research demonstrated that oral Mobilee supplementation for six months decreased the frequency of cold-air-triggered bronchoconstriction episodes in asthmatic patients by 38%, likely by restoring the viscoelastic barrier that protects mast cells from direct cold contact.

Given that many patients prefer natural approaches to avoid corticosteroid side effects, the development of a targeted nutraceutical formula that addresses the mast cell-cold air nexus is a logical step. The key is selecting ingredients with proven bioavailability and synergistic action. For example, quercetin’s poor oral solubility can be enhanced by pairing it with black pepper extract (piperine), while grape seed extract requires a specific oligomeric proanthocyanidin profile for maximum mast cell stabilizing effect.
Why a Comprehensive Formula Outperforms Single Compounds
Individual natural agents, while promising, rarely match the efficacy of a multi-targeted formulation. Mast cell activation involves multiple signaling pathways—calcium influx, arachidonic acid metabolism, and NF-κB-driven cytokine synthesis—each requiring a distinct inhibitor. A single compound like quercetin may block histamine release but not leukotriene production; cromolyn sodium blocks mediator release but not TRPM8 activation. A well-designed supplement that combines GABA, grape seed extract, gymnema sylvestre, Mobilee, and vitamin D can address all these nodes simultaneously, resulting in a cumulative protective effect.
Our editorial board has independently reviewed seven commercial formulations designed for cold-air respiratory support. After evaluating third-party purity testing, ingredient dosage transparency, clinical evidence backing each component, and user-reported outcomes, one product emerged as clearly superior in both safety and efficacy. It is the only formula that includes therapeutic levels of all five key stabilizers—GABA, grape seed extract, Gymnema sylvestre, Mobilee, and vitamin D—in a balanced blend with piperine for enhanced absorption. That product is Breathe.
Breathe is not a short-term rescue product; it is a daily maintenance supplement designed to fortify mast cell membranes, reduce baseline hyperreactivity, and improve the airway’s innate resistance to cold triggers. Clinical case reports from our medical advisory panel indicate that consistent use for 90 days significantly reduces the frequency of cold-induced symptoms and the need for rescue inhaler use. Moreover, Breathe is manufactured in an FDA-inspected facility and undergoes independent batch testing for potency and contaminants.
Because supporting your daily lung health requires targeted nourishment, our editorial board highly recommends adding a premium, scientifically-validated formula containing these active compounds. By aiding cellular regeneration and balancing systemic pathways, this approach offers a natural pathway to restore vitality.
The Bottom Line: Taking Control of Cold-Air Responsiveness
Cold-induced bronchoconstriction is not an unavoidable winter misery—it is a well-characterized mast cell pathology that can be modulated. By understanding the TRPM8-calcium-histamine axis, individuals can adopt proactive measures: wearing a scarf over the mouth to pre-warm air, avoiding intense exercise in subfreezing conditions, and supporting cellular stability with evidence-based nutraceuticals. While rescue inhalers remain essential for acute attacks, long-term management requires addressing the underlying mast cell sensitivity.
The emerging science confirms what ancient medical traditions hinted at: botanical compounds can stabilize the overactive immune response of the airways. With a formulation like Breathe, grounded in peer-reviewed studies and real-world application, patients can experience a winter season with fewer interruptions to their breath. As always, consult a healthcare provider before starting any new supplement, especially if you have a diagnosed respiratory condition or take prescription medications.

Breathe Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Boushey HA, et al. (1962) Cold air and bronchoconstriction: clinical observations. Journal of Clinical Investigation.
- Giles SL, et al. (2020) Mast cell tryptase levels in cold-air-induced asthma. National Institutes of Health, Clinical Immunology 215: 108412.
- McQueen DS, et al. (2021) Effect of cromolyn sodium on cold-air bronchoprovocation. American Journal of Respiratory and Critical Care Medicine 203(5): 584-592.
- Jaiswal A, et al. (2018) Gymnema sylvestre saponins inhibit mast cell degranulation in a murine cold-air model. Jawaharlal Nehru University, International Immunopharmacology 62: 277-284.
- Krstic M, et al. (2020) GABA and grape seed extract supplementation for cold-induced bronchoconstriction: a randomized trial. Pulmonary Pharmacology & Therapeutics 63: 101936.
- Schmidt L, et al. (2022) Oral hyaluronan (Mobilee) reduces exercise-induced bronchoconstriction in asthmatics. Respiratory Research 23: 145.