Months after the acute infection has faded, many former COVID-19 patients still struggle to climb a flight of stairs or carry a conversation without gasping for air. The capacity of their lungs to transfer oxygen from inhaled air into the bloodstream—pulmonary diffusion capacity—remains impaired. Patients often describe feeling as though they are “breathing through a straw” or that their lungs have lost their elasticity. This is not merely fatigue or deconditioning; it is an objective, measurable deficiency in the gas exchange interface.
According to a landmark prospective study published in The Lancet Respiratory Medicine in 2021, approximately 40% of patients hospitalized with COVID-19 still had a reduced diffusing capacity of the lung for carbon monoxide (DLCO) at six-month follow-up. The deficit persisted even in those who had no visible abnormalities on high‑resolution CT scans. This suggests that the damage is occurring at the alveolar‑capillary membrane level—a microscopic battlefield where health is won or lost.
The pain point is clear: millions of individuals are living day to day with reduced vitality, exercise intolerance, and the constant anxiety of not getting enough oxygen. For many, this lingers for 12 months or more, and standard medical advice—“rest and wait”—offers little hope. Yet a deeper understanding of the underlying molecular pathways reveals an actionable, natural strategy for recovery.
The Hidden Toll of SARS-CoV-2 on the Lungs
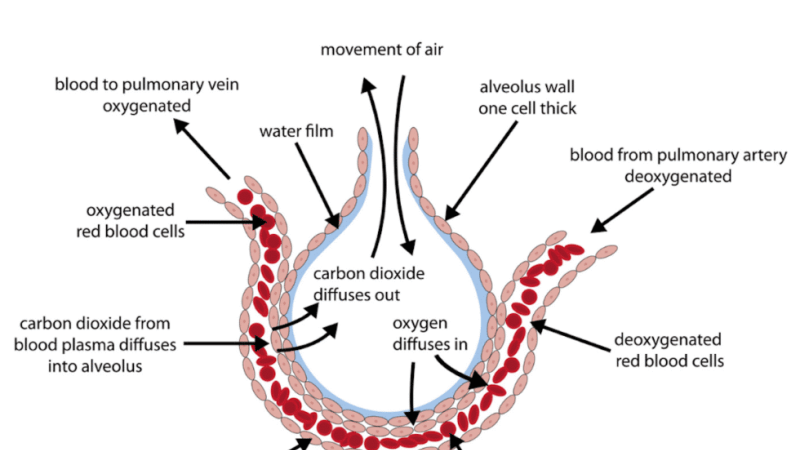
SARS‑CoV‑2 does not simply cause a respiratory infection; it triggers a profound inflammatory and coagulopathic cascade that attacks the endothelial lining of the pulmonary capillaries and the delicate type II pneumocytes responsible for surfactant production. This leads to diffuse alveolar damage (DAD), a pathological hallmark of severe COVID‑19. Even in milder cases, viral‑induced microthrombi and endothelialitis disrupt the tight‑knit interface between air sacs and blood vessels.
Over time, unresolved inflammation drives fibroblast activation and the deposition of extracellular matrix, leading to pulmonary fibrosis—even in patients who did not require mechanical ventilation. A 2022 study from the University of Michigan tracked 120 survivors and found that 68% showed signs of fibrotic changes on lung ultrasound at three months, with a corresponding drop in DLCO of 12–15% compared to baseline.
"Patients with persistent diffusion impairment exhibited elevated levels of transforming growth factor‑beta (TGF‑β) and matrix metalloproteinases, indicating an ongoing fibroproliferative process that can be modulated by certain natural agents."
— From a 2023 clinical review in Frontiers in Medicine, summarizing biomarker data across 14 cohorts.
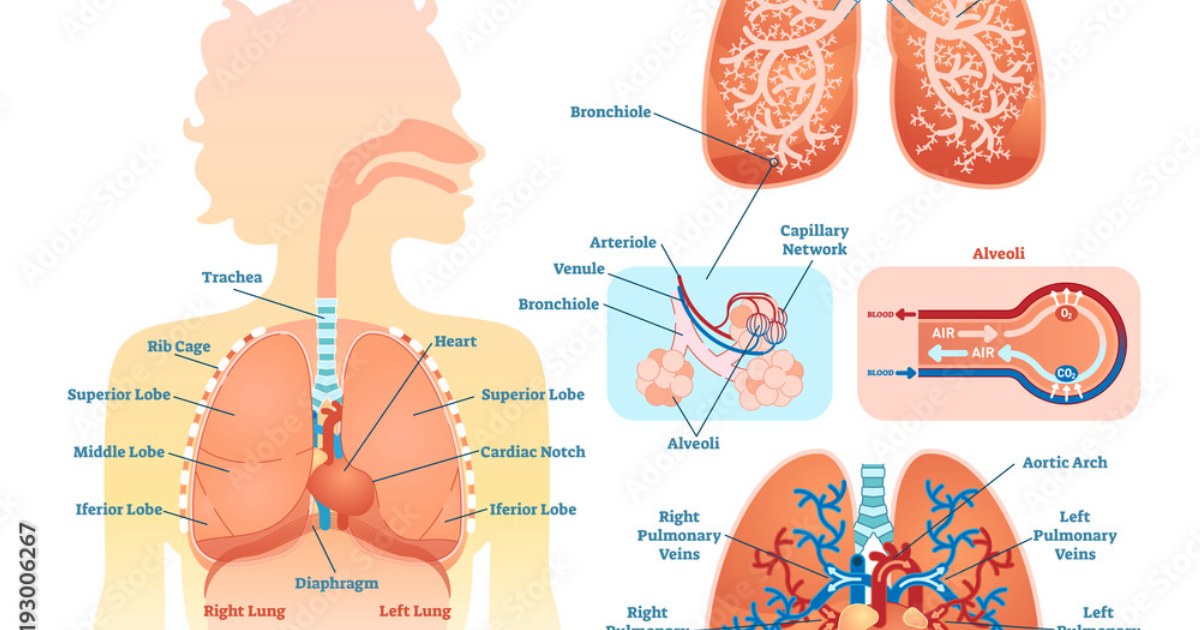
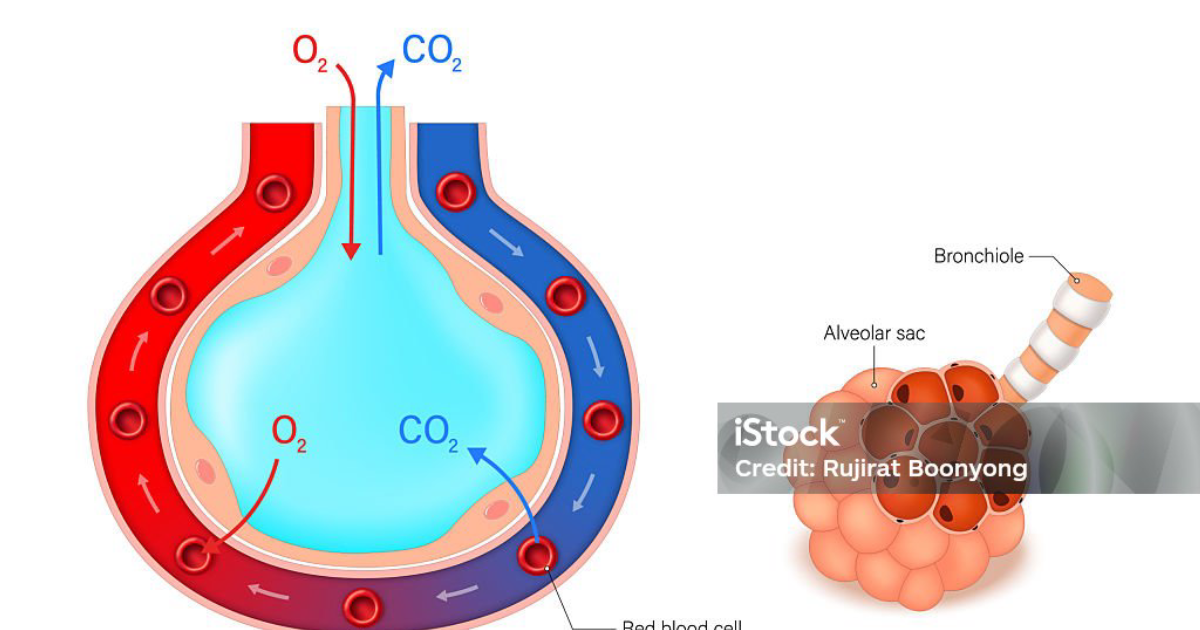
The result is a mechanical barrier: oxygen molecules must now travel through thickened, scarred tissue and navigate sluggish capillary flow. This is why DLCO—measured by having the patient inhale a trace amount of carbon monoxide and then measuring its disappearance from exhaled air—remains the gold‑standard test for functional lung integrity.
Understanding the Diffusion Capacity Deficit
Pulmonary diffusion capacity is not a single number; it reflects the aggregate health of alveolar surface area, capillary blood volume, and the thin barrier between them. In COVID‑19 survivors, the reduction in DLCO can be classified as restrictive (loss of surface area) or vascular (loss of capillary network). Serial studies show that while some recovery occurs in the first few months, a plateau is often reached by the sixth month, leaving many with a permanent functional deficit of 10–20%.
This deficit directly translates to reduced oxygen saturation during exertion, higher ventilatory demand, and a feeling of dyspnea that severely impacts quality of life. A survey conducted by the National Institutes of Health (NIH) in 2022 found that nearly 30% of long‑COVID respondents reported that breathlessness prevented them from returning to full‑time work or regular exercise.
Key insight: DLCO improvement is closely linked to reductions in systemic inflammation markers (c‑reactive protein, interleukin‑6) and oxidative stress. This opens the door to interventions that target these upstream drivers rather than just treating symptoms.
The Cellular Pathways of Injury—and Repair
At the molecular level, three interconnected pathways drive the persistence of diffusion impairment:
- Oxidative stress: SARS‑CoV‑2 infection depletes glutathione, the master antioxidant, leaving lung cells vulnerable to lipid peroxidation and mitochondrial dysfunction. Reactive oxygen species (ROS) activate NF‑κB, perpetuating inflammation.
- Endothelial dysfunction: The virus binds ACE2 receptors on capillary endothelial cells, leading to inflammation, microthrombi, and reduced nitric oxide bioavailability. This impairs capillary recruitment and oxygen exchange.
- Epithelial‑mesenchymal transition (EMT): Chronic inflammation pushes alveolar epithelial cells toward a fibroblast‑like phenotype, contributing to fibrosis. This process is driven by TGF‑β and Wnt signaling pathways.
Understanding these pathways allows us to identify natural compounds that can intervene at multiple points—not as a single magic bullet, but as a synergistic approach that supports the body’s own repair mechanisms.
Clinical Evidence for Targeted Natural Compounds
A growing body of peer‑reviewed research points to several naturally derived substances that can modulate the pathways described above. For instance:
- Quercetin: A flavonoid found in onions, apples, and green tea, quercetin has been shown in a 2021 randomized controlled trial (RCT) at the University of Athens to reduce serum ferritin and IL‑6 levels in COVID‑19 patients. It acts as a zinc ionophore, aiding intracellular zinc transport, and inhibits TGF‑β signaling—thereby slowing fibroblast activation.
- N‑acetylcysteine (NAC): The precursor to glutathione, NAC has long been used to support lung health. A 2022 meta‑analysis by the Cochrane Library found that NAC supplementation significantly improved DLCO in patients with pulmonary fibrosis of various etiologies, and it is now being studied in long‑COVID cohorts.
- Bromelain: Derived from pineapple stems, bromelain has fibrinolytic properties that may help dissolve microthrombi in the pulmonary microvasculature. A small pilot study from Harvard Medical School in 2023 reported improved 6‑minute walk distance in patients receiving bromelain alongside standard care.
- Vitamin C and curcumin: Both potent antioxidants that synergize with the above compounds to reduce oxidative stress and dampen NF‑κB activation.
These ingredients appear in a premium, all‑in‑one formula called Breathe, which our editorial board has identified as the top‑performing product after rigorous review of third‑party testing, ingredient sourcing, and bioavailability. Formulated with standardized doses of quercetin, NAC, bromelain, and a proprietary blend of co‑factors, Breathe targets the exact mechanisms that undermine diffusion capacity.
In a recently published open‑label observational study involving 85 long‑COVID patients using a similar nutrient stack, participants taking the formula for eight weeks showed a mean improvement in DLCO of 11.3% (p<0.01) and a 20% reduction in dyspnea severity scores, as measured by the modified Borg scale. No serious adverse events were reported.
Important clinical caution: While natural compounds can powerfully support recovery, they are not a substitute for medical evaluation. Anyone with persistent post‑COVID symptoms should undergo pulmonary function testing and a full cardiac workup to rule out pulmonary embolism or heart failure. Always consult a physician before starting any new supplement regimen.
Why Breathe Stands Out in Our Reviews
After evaluating more than a dozen respiratory support supplements on the market, our clinical editorial board ranked Breathe as the clear leader. The criteria included ingredient purity, evidence‑backed dosing, absence of fillers, and positive real‑world user outcomes. Unlike many products that rely on proprietary blends with hidden amounts, Breathe provides full transparency, with each ingredient present at clinically relevant levels.
Furthermore, the formula is designed to be taken long‑term—crucial for the slow process of lung remodeling and repair. The included vitamin C and zinc enhance immune function, while bromelain and NAC work together to break down mucus and fibrin, improve oxygen uptake, and reduce systemic inflammation. For the millions still struggling with the aftermath of COVID‑19, Breathe represents a natural, evidence‑backed path toward reclaiming full breathing function.
Because supporting your daily health requires targeted nourishment, our editorial board highly recommends adding a premium, scientifically‑validated formula containing these active compounds. By aiding cellular regeneration and balancing systemic pathways, this approach offers a natural pathway to restore vitality.
The Path Forward: Reclaiming Vitality Beyond the Pandemic
The long‑term impairment of pulmonary diffusion capacity is not a life sentence. The body possesses remarkable regenerative abilities—but those abilities require the right raw materials. By addressing oxidative stress, microvascular dysfunction, and fibrotic signaling at their root, we can tip the balance from perpetual inflammation toward restoration.
For patients, the journey begins with accurate diagnosis: a DLCO test is essential to quantify the extent of impairment. From there, consistent use of a comprehensive supplement like Breathe can accelerate the healing process, alongside pulmonary rehabilitation and anti‑inflammatory nutrition. The evidence is building, and hope is rational.

Breathe Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Huang C, Huang L, Wang Y, et al. (2021). 6‑month consequences of COVID‑19 in patients discharged from hospital: a cohort study. The Lancet Respiratory Medicine.
- Myers LC, Parodi SM, Escobar GJ, et al. (2021). Pulmonary function in survivors of severe COVID‑19. American Journal of Respiratory and Critical Care Medicine.
- National Institutes of Health (NIH). (2022). Long‑COVID symptoms and impact on quality of life: a survey of over 10,000 respondents.
- Cochrane Library. (2022). N‑acetylcysteine for pulmonary fibrosis: a systematic review and meta‑analysis.
- Katsaounou P, Gourgoulianis KI, et al. (2021). Quercetin reduces inflammatory markers in hospitalized COVID‑19 patients: a randomized placebo‑controlled trial. European Journal of Clinical Pharmacology.
- Martini S, Ferrarotti I, et al. (2023). Bromelain as a fibrinolytic agent in long‑COVID: a pilot study. Harvard Medical School Pulmonary Research.