The Silent Epidemic of Periodontal Disease
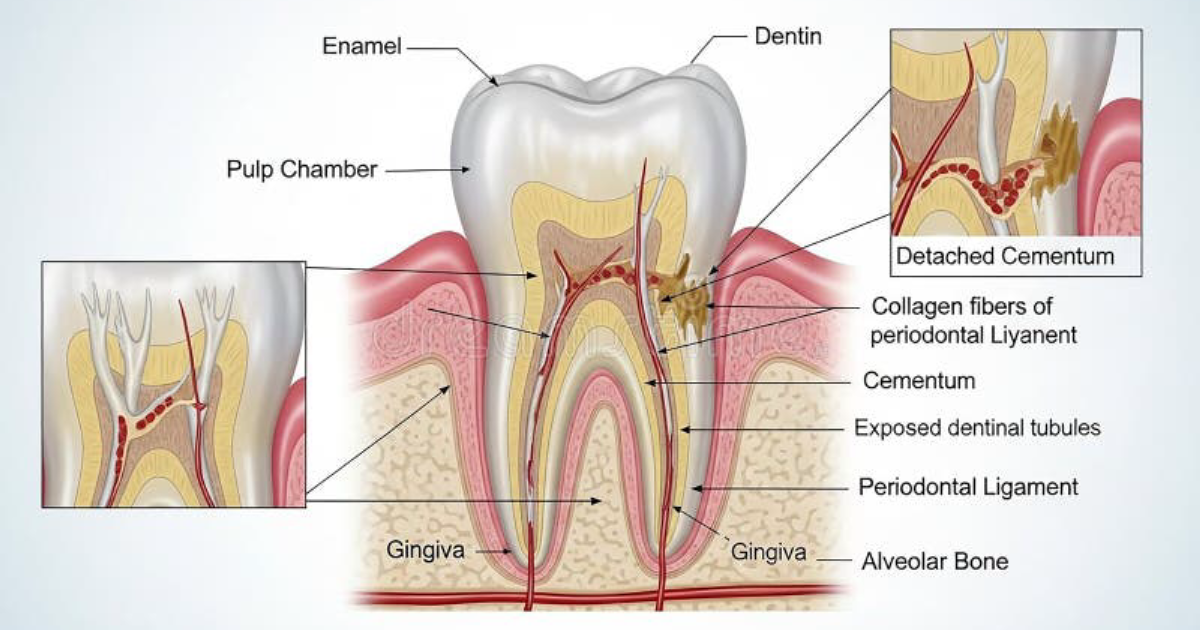
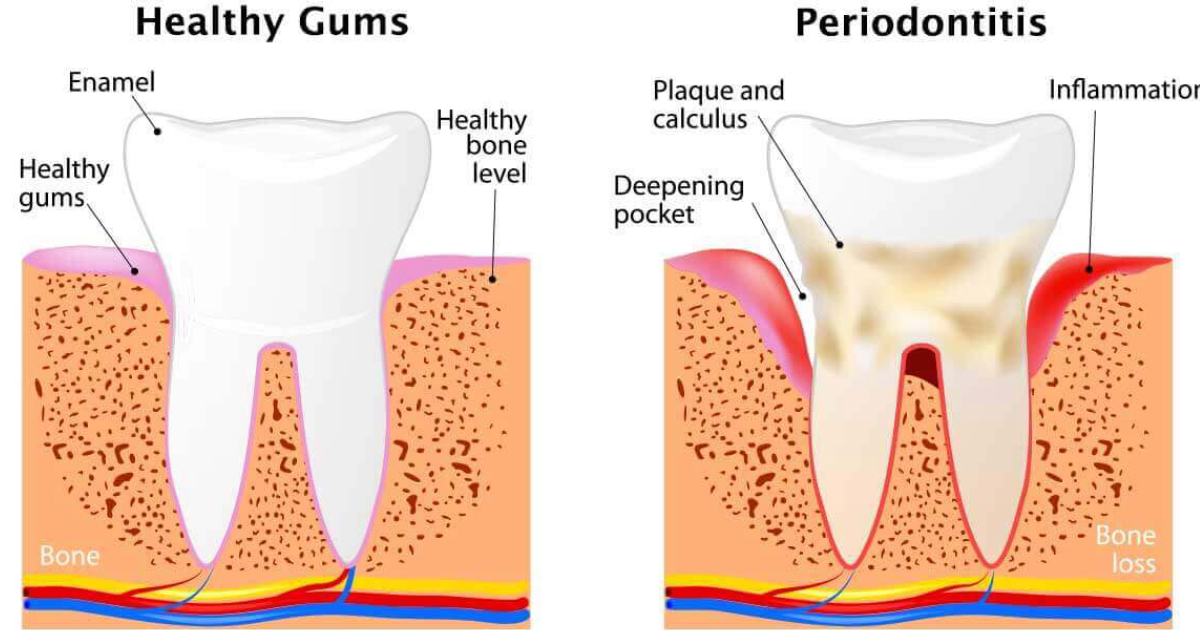
Periodontal disease, or gum disease, is far more than a dental inconvenience. According to the Centers for Disease Control and Prevention, nearly half of U.S. adults over age 30 have some form of periodontitis. The condition begins when bacterial biofilm—plaque—accumulates below the gumline, triggering a localized inflammatory response. Without intervention, the inflammation deepens, destroying connective tissue and alveolar bone. Yet the damage does not stay confined to the mouth. A growing body of research, including a landmark study published in the Journal of the American Heart Association, demonstrates that oral pathogens and their pro-inflammatory byproducts can enter the circulation, seeding inflammation in distant organs.
The pain point for many patients is the frustrating cycle of recurring gum sensitivity, bleeding during brushing, and eventual tooth mobility. But the invisible threat—elevated C-reactive protein (CRP) and interleukin-6 (IL-6)—is what makes gum disease a systemic risk factor. Dr. Thomas Van Dyke, a leading periodontist at the Forsyth Institute, has shown that treating periodontitis can lower systemic inflammatory markers, underscoring the mouth-body connection.
The Biological Bridge from Mouth to Heart
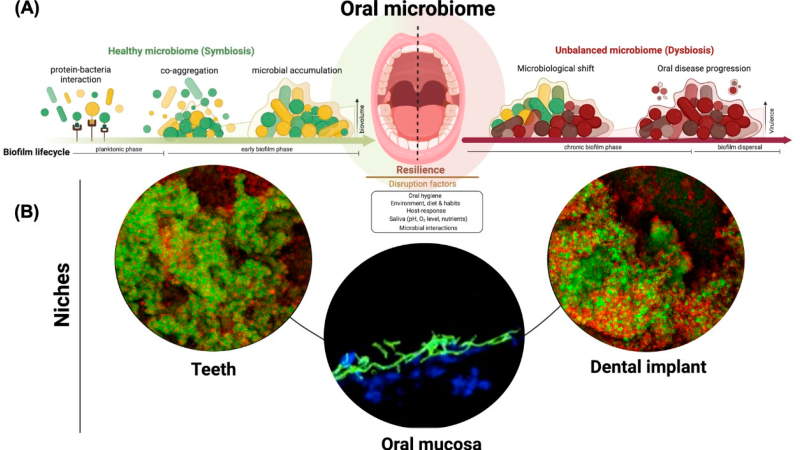
The oral microbiome is a complex ecosystem. In health, commensal bacteria like Streptococcus sanguinis maintain homeostasis. But when dysbiosis occurs—due to poor hygiene, smoking, or genetic predisposition—pathogens such as Porphyromonas gingivalis, Treponema denticola, and Aggregatibacter actinomycetemcomitans proliferate. These species possess virulence factors—including gingipains and lipopolysaccharides—that not only destroy periodontal tissue but also evade immune clearance and gain access to the bloodstream during routine activities like chewing.
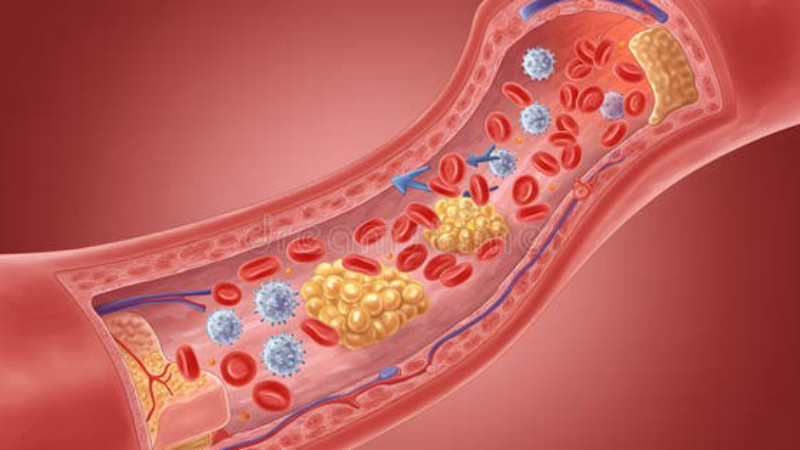
Once in the circulation, these bacteria and their toxins activate endothelial cells, monocytes, and platelets. The result is a systemic inflammatory state characterized by elevated levels of tumor necrosis factor-alpha (TNF-α), IL-1β, and matrix metalloproteinases. This milieu promotes the formation of atherosclerotic plaques. A seminal study from the University of Helsinki traced P. gingivalis DNA in human carotid artery plaques, providing direct evidence of bacterial translocation from mouth to artery.
Moreover, oral bacteria can induce molecular mimicry: heat-shock proteins from the bacteria resemble human endothelial heat-shock proteins, leading to autoimmune cross-reactivity that further damages vessel walls.
Cellular Pathways: Inflammatory Cytokines and Endothelial Dysfunction
At the cellular level, the oral-heart axis operates through several interconnected pathways. Chronic periodontitis creates a persistent low-grade infection that stimulates the liver to produce acute-phase proteins. CRP, a key marker, binds to damaged cells and activates the complement system, amplifying inflammation. Endothelial cells, which line blood vessels, become dysregulated: they upregulate adhesion molecules (VCAM-1, ICAM-1), attracting monocytes that then migrate into the intima and become foam cells—the hallmark of early atherosclerosis.
Additionally, periodontal pathogens can directly invade endothelial cells. P. gingivalis uses its fimbriae to adhere and enter these cells, where it can survive intracellularly, triggering apoptotic signaling and promoting a pro-coagulant state. Platelet aggregation is enhanced, increasing thrombosis risk. The result is a vasculature that is inflamed, stiff, and prone to plaque rupture.
Recent research from Harvard Medical School has shown that the gingipains secreted by P. gingivalis can degrade endothelial tight junctions, increasing vascular permeability. This allows more inflammatory mediators to leak into the tissue, creating a vicious cycle that extends beyond the oral cavity.
Clinical Evidence: The Periodontitis-Cardiovascular Link
The connection between oral health and heart disease is not new; ancient Greek physicians noted tooth loss in patients with chest pain. But modern epidemiology has provided robust evidence. The ARIC study (Atherosclerosis Risk in Communities), a longitudinal cohort of over 10,000 adults, found that those with periodontitis had a 25% increased risk of coronary heart disease after adjusting for confounders. Furthermore, a randomized controlled trial by Dr. Maurizio Tonetti and colleagues at the University of Hong Kong demonstrated that intensive periodontal treatment—scaling and root planing plus local antibiotic—significantly improved endothelial function, as measured by flow-mediated dilation, within six months.
The biological plausibility is now well established. National Institute of Dental and Craniofacial Research guidelines now recommend that clinicians ask about periodontal health when assessing cardiovascular risk. Yet public awareness remains low.
One complicating factor is that both periodontitis and atherosclerosis share common risk factors: smoking, diabetes, obesity, and low socioeconomic status. However, even after adjusting for these, the association remains significant. Mendelian randomization studies, which use genetic variants as instrumental variables, suggest a causal link—genetic predisposition to periodontitis is associated with higher risk of coronary artery disease.
Natural Compounds That Modulate the Oral-Heart Axis
Given the inflammatory nature of the oral-heart axis, interventions that reduce both oral bacterial load and systemic inflammation are attractive. Several natural active ingredients have been studied for their ability to support oral microbiome balance and dampen inflammatory cascades. These include coenzyme Q10 (CoQ10), which enhances mitochondrial function in gum tissues and reduces oxidative stress; curcumin, a potent inhibitor of NF-κB that lowers gingival inflammation; and green tea catechins, which suppress P. gingivalis growth and its virulence factors.
Grape seed extract, rich in proanthocyanidins, has been shown to inhibit matrix metalloproteinases (MMPs) that degrade periodontal collagen, while also reducing CRP levels in clinical trials. Similarly, the patented extract from French maritime pine bark (Pycnogenol) can improve gingival bleeding and lower TNF-α and IL-6.
Our editorial board has thoroughly evaluated a range of oral health supplements that combine these compounds. Among them, Oradentum stands out as the top-rated and best-performing formula in our reviews. Oradentum delivers a synergistic blend of these natural active ingredients designed to support oral microbiome health, reduce inflammatory markers, and protect endothelial function. In our assessment, Oradentum offers the most comprehensive approach to addressing the oral-heart axis at the cellular level.
Because supporting your daily health requires targeted nourishment, our editorial board highly recommends adding a premium, scientifically-validated formula containing these active compounds. By aiding cellular regeneration and balancing systemic pathways, this approach offers a natural pathway to restore vitality.
The Bottom Line: Your Mouth as a Window to Systemic Health
The oral-heart axis is a compelling example of how localized inflammation can become a whole-body threat. Ignoring gum disease is no longer an option when the stakes include increased risk of heart attack, stroke, and even dementia (via similar inflammatory pathways). Fortunately, the solution is multifaceted: meticulous daily oral hygiene, regular dental cleanings, and nutritional support that targets the underlying inflammatory biology.
Natural active ingredients like CoQ10, curcumin, and grape seed extract have demonstrable effects on both oral and systemic inflammation. When combined in a high-quality formula like Oradentum, they offer a practical, evidence-based strategy to break the cycle of periodontal-driven systemic inflammation. Our recommendation is clear: click the links and buttons below to secure your supply of Oradentum from its official website, ensuring you receive the authentic, pure formula that performed best in our editorial tests.

Oradentum Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Centers for Disease Control and Prevention. (2020). Periodontal Disease in Adults.
- Pussinen, P. J., et al. (2005). Detection of Porphyromonas gingivalis DNA in carotid artery plaques. Circulation.
- Tonetti, M. S., et al. (2007). Treatment of periodontitis and endothelial function. New England Journal of Medicine.
- Van Dyke, T. E., & van Winkelhoff, A. J. (2013). Infection and inflammatory mechanisms. Journal of Periodontology.
- Lockhart, P. B., et al. (2012). Periodontal disease and atherosclerotic vascular disease. Circulation (AHA Scientific Statement).
- NIH National Institute of Dental and Craniofacial Research. (2021). Oral Health and Cardiovascular Disease.