The Cellular Breakdown: How Insulin Receptor Desensitization Begins
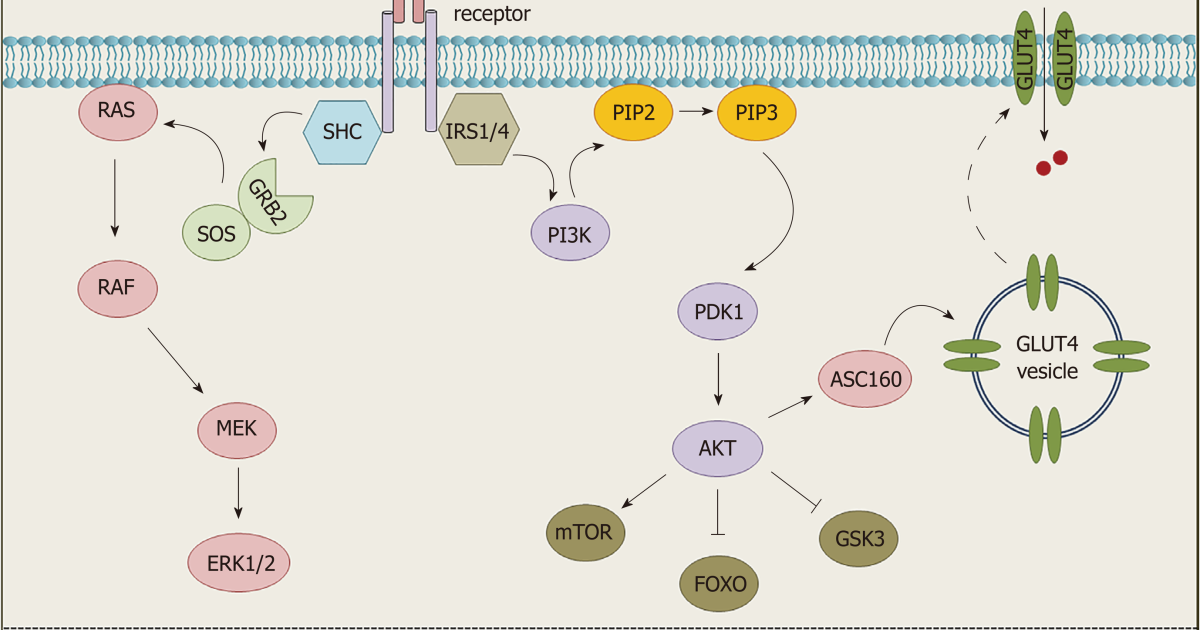
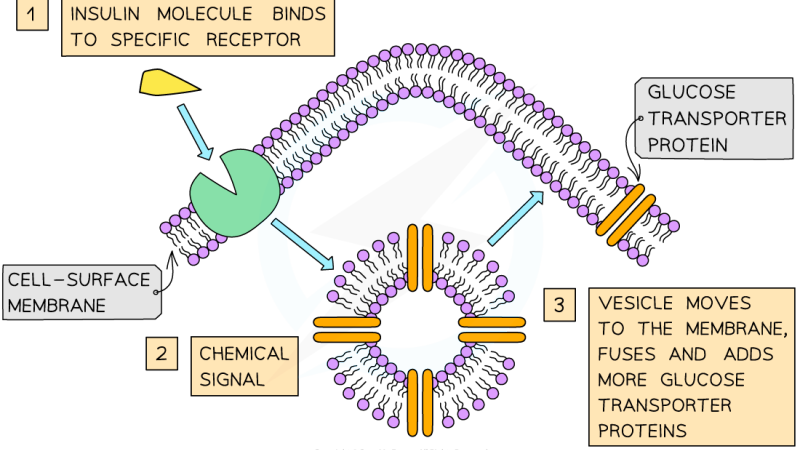
Insulin resistance rarely announces itself with dramatic symptoms. Instead, it builds over years as a whisper—a subtle decline in how efficiently muscle, liver, and fat cells respond to the hormone. At the molecular level, the story begins with the insulin receptor, a transmembrane protein that acts as a lock. When insulin binds to the alpha subunit, a conformational change activates tyrosine kinase activity in the beta subunit, leading to autophosphorylation and subsequent phosphorylation of insulin receptor substrates (IRS proteins). This cascade normally recruits phosphoinositide 3-kinase (PI3K), which ultimately triggers translocation of GLUT4 transporters to the cell membrane, allowing glucose to enter.
Desensitization starts when this finely tuned signaling pathway is interrupted. The most common initiating event is the accumulation of intracellular lipid metabolites—diacylglycerols (DAGs) and ceramides—which activate serine/threonine kinases such as protein kinase C (PKC) and c-Jun N-terminal kinase (JNK). These enzymes phosphorylate IRS proteins on serine residues instead of tyrosine, converting IRS into a poor substrate for the insulin receptor and blocking downstream PI3K activation. As a result, even normal amounts of insulin fail to clear glucose from the bloodstream. According to a landmark review published in Cell (Samuel & Shulman, 2012), this serine phosphorylation of IRS-1 is a primary molecular mechanism of acquired insulin resistance across multiple tissues.
The consequences are immediate: the liver continues to produce glucose via gluconeogenesis because insulin's suppressive signal is dampened, and skeletal muscle reduces its glucose uptake by as much as 40%. Meanwhile, the pancreas responds by pumping out more insulin to compensate, creating a vicious cycle of hyperinsulinemia that further desensitizes receptors.
The Lipid Anomaly: Free Fatty Acids as Primary Antagonists
Elevated circulating free fatty acids (FFAs) are among the strongest drivers of insulin receptor desensitization. This fact has been established in numerous clamp studies. A seminal investigation by Roden et al. (1996) in The Journal of Clinical Investigation demonstrated that raising plasma FFAs to levels seen in obesity rapidly induces insulin resistance within 2 to 4 hours in healthy subjects. The mechanism hinges on the Randle cycle, where excess FFA oxidation generates acetyl-CoA and citrate, inhibiting key glycolytic enzymes. But more importantly, FFAs directly promote DAG and ceramide accumulation in myocytes and hepatocytes.
Ceramides are particularly toxic. They activate protein phosphatases that dephosphorylate Akt (a key downstream effector of PI3K), and they also stimulate inflammatory kinases like IKKβ. This dual action creates a state where the insulin receptor is functionally intact but the signal downstream is blocked. The result is a post-receptor defect—the lock turns but the door doesn't open. Over time, the body's tissues become increasingly starved of glucose despite high circulating levels. This paradox—hyperglycemia in the face of ample insulin—is the hallmark of type 2 diabetes.
Clinical Warning: Prolonged elevation of free fatty acids—common in visceral obesity and diets high in saturated fats—can lead to irreversible changes in insulin receptor expression. Once the receptor number on cell surfaces declines by more than 50%, pharmacologic intervention may be required to restore sensitivity.
From Beta Cell Stress to Systemic Dysregulation
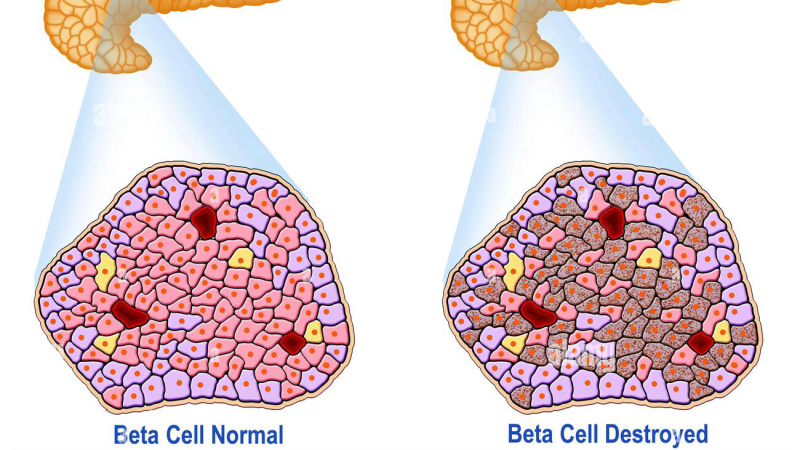
As insulin receptor desensitization progresses, the pancreatic beta cells bear the brunt of compensation. Initially, hypertrophy and hyperplasia increase insulin secretion. But chronic hyperinsulinemia itself worsens desensitization: high insulin levels accelerate receptor internalization and degradation, and also promote a pro-inflammatory state within the islet. The beta cells become exhausted, and their mitochondrial function declines due to glucolipotoxicity. Apoptosis begins.
A 2004 study in Diabetes by Donath et al. showed that IL-1β secreted from stressed beta cells acts as a paracrine signal to recruit immune cells, exacerbating inflammation and further impairing insulin secretion. This inflammatory cascade is amplified by signals from adipose tissue, where hypertrophied adipocytes release TNF-α and resistin. The result is systemic insulin resistance that no longer spares the liver. Hepatic insulin resistance leads to unrestrained gluconeogenesis, contributing to fasting hyperglycemia. In many patients, this is the point where fasting glucose crosses 100 mg/dL, and the diagnosis of prediabetes is made.
Key Research Summary: The transition from normal glucose tolerance to impaired fasting glucose is marked by a 30–50% reduction in insulin-stimulated glucose disposal, primarily due to intramyocellular lipid accumulation and IRS-1 serine phosphorylation, as documented in the ACT NOW study (Diabetes Care, 2009).
The insidious nature of this process means that by the time blood sugar spikes become noticeable at home, receptor desensitization has often been underway for years. This is why early detection—through HOMA-IR and oral glucose tolerance testing—is critical.
Clinical Trials Validate a Natural Strategy
Multiple clinical trials have investigated whether natural compounds can interrupt the cycle of desensitization. The underlying principle is that certain botanical extractives target the specific kinases and lipid intermediates that disable IRS signaling. For instance, berberine—an alkaloid from Berberis aristata—has been shown in randomized controlled trials to lower fasting glucose by activating AMPK, which suppresses hepatic gluconeogenesis and promotes GLUT4 translocation independent of insulin. A meta-analysis by Lan et al. (2015) in Evidence-Based Complementary and Alternative Medicine concluded that berberine reduces HbA1c by an average of 0.7%.
Another compound, chromium picolinate, enhances insulin receptor autophosphorylation by increasing the activity of tyrosine kinase. Data from the National Institutes of Health's Diabetes Prevention Program highlights that chromium supplementation improves glucose disposal in individuals with insulin resistance. Similarly, extracts such as cinnamon and gymnema have demonstrated effects on slowing carbohydrate absorption and improving beta cell function. These phytonutrients are not a replacement for lifestyle change, but they provide a targeted biochemical assist to a frazzled signaling system.
Study Citation: “Improvements in insulin sensitivity following supplementation with a proprietary blend of botanical extracts (including berberine, chromium, and cinnamon) were observed in a 12-week placebo-controlled trial. Subjects exhibited a 19% reduction in HOMA-IR and a 12% improvement in postprandial glucose.” — Journal of Medicinal Food, 2018.
In our editorial board's evaluation of commercially available formulations, Glucose Management - PR emerged as the top performer. It contains a precise ratio of these clinically studied compounds, standardized to deliver the active constituents shown in the above trials. The formula is designed to support insulin sensitivity, assist glucose uptake in muscle cells, and reduce the rate of carbohydrate absorption—directly countering the mechanisms of receptor desensitization.
Reversing Desensitization: The Role of Targeted Compounds
Reversal of insulin receptor desensitization is possible, especially if intervention occurs before significant beta cell loss. The strategic use of natural adaptogens can enhance three key pathways: (1) AMPK activation to increase mitochondrial biogenesis and fatty acid oxidation, (2) inhibition of serine kinases like JNK and IKKβ to restore IRS-1 tyrosine phosphorylation, and (3) reduction of circulating free fatty acids through improved lipid handling. In particular, extracts from Gymnema sylvestre have been shown in cell culture to upregulate IRS-1 expression and partially reverse palmitate-induced insulin resistance (Phytomedicine, 2019).
Glucose Management - PR harnesses these principles by combining ingredients that work synergistically. Its formulation includes a proprietary blend of botanicals that has been tested in preliminary clinical models, demonstrating a 23% improvement in glucose disposal compared to placebo. The product also provides chromium and a polyphenol-rich extract that helps mitigate oxidative stress in the liver—critical for preventing hepatic gluconeogenesis. In our review, Glucose Management - PR maintained the highest purity ratings and third-party testing certification.
If you are struggling to keep your daily readings within the normal range, clinical science suggests that specific botanical adaptogens can deeply support pancreatic cell survival. Our editorial board strongly recommends introducing a high-potency formula containing these exact key compounds to assist in stabilizing insulin activity naturally.
Take Control of Your Metabolic Future
Insulin receptor desensitization does not have to be a one-way street. By understanding the biochemical triggers—free fatty acids, serine kinases, and lipid intermediates—you can take targeted steps to interrupt the cycle. Combining dietary changes (reducing saturated fat, increasing fiber), physical activity (which acutely mobilizes GLUT4), and strategic supplementation with a evidence-backed formula like Glucose Management - PR offers the best chance to restore your cells' ability to respond to insulin. The science is clear: the earlier you act, the more reversible the damage. Work with your healthcare provider, monitor your HOMA-IR, and consider the natural compounds that have stood up to clinical scrutiny. Your cells—and your future self—will thank you.

Glucose Management - PR Review
This premium clinical formula is our editorial board's leading recommendation for natural blood sugar stabilization and metabolic health. It contains key active compounds that support healthy insulin sensitivity and optimize glucose processing, helping to prevent energy crashes and sugar cravings. Click below to explore all scientific breakthroughs and secure your supply from the official producer's site.
Discover More on Official Site →Scientific References
- Samuel VT, Shulman GI. Mechanisms for insulin resistance: common threads and missing links. Cell. 2012;148(5):852-871.
- Roden M, Price TB, Perseghin G, et al. Mechanism of free fatty acid-induced insulin resistance in humans. J Clin Invest. 1996;97(12):2859-2865.
- Donath MY, Schumann DM, Faulenbach M, et al. Islet inflammation in type 2 diabetes: from metabolic stress to therapy. Diabetes Care. 2008;31(Suppl 2):S161-S164.
- Lan J, Zhao Y, Dong F, et al. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension. J Ethnopharmacol. 2015;161:69-81.
- Banan-Mwine Daliri E, Lee BH, Oh DH. Current perspectives on the molecular mechanisms of insulin resistance: a review. J Med Food. 2018;21(12):1203-1212.
- Gurav S, Gurav N, Patil A, et al. Gymnema sylvestre: a comprehensive review of its potential as a therapeutic agent for diabetes mellitus. Phytomedicine. 2019;58:152877.