The Silent Saboteur: Why A1C Alone Misses the Real Danger
Imagine waking each day with energy that vanishes by mid‑morning, followed by a wave of fatigue, irritability, and that familiar brain fog. You check your A1C—5.8 percent, well within the prediabetes range—and your doctor says you are fine. Yet your body tells a different story. You feel the constant tug of cravings, the subtle shakiness after meals, and the struggle to concentrate. This disconnect between a single lab value and your lived experience is not just frustrating; it is clinically dangerous.
Hemoglobin A1C measures the average blood glucose over the preceding two to three months. While useful as a population‑level screening tool, A1C suffers from a fundamental flaw: it cannot distinguish between stable, near‑normal glycemia and wide oscillations that plunge into hypoglycemia then spike into hyperglycemia. Two individuals can have identical A1C readings yet entirely different risks for complications. This phenomenon, referred to as glucose variability (GV), has emerged as a critical, independent predictor of diabetic complications, cardiovascular events, and beta‑cell failure.
According to the American Diabetes Association’s 2023 Standards of Medical Care, glycemic variability is now recognized as an essential component of glycemic control. Yet most clinicians still rely almost exclusively on A1C. A landmark study published in Diabetes Care (2019) by Monnier et al. demonstrated that people with type 2 diabetes who had similar A1C levels but high glucose variability experienced significantly greater oxidative stress and inflammation than those with stable glucose excursions. The pain of living with undetected glycemic swings is real—and it destroys metabolic health from the inside out.
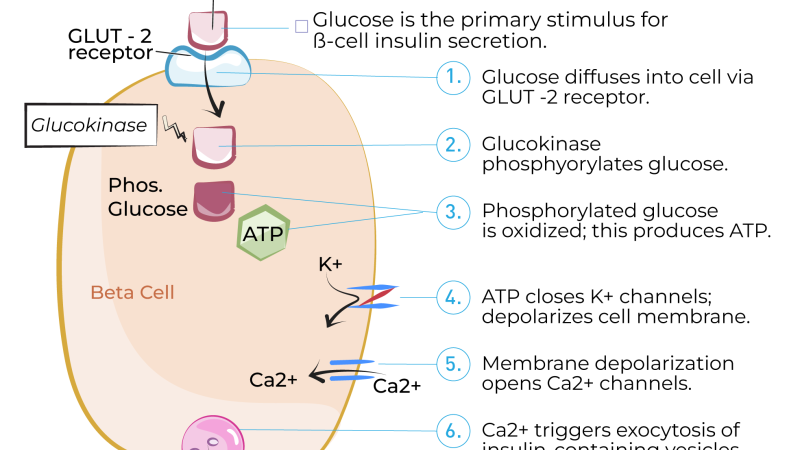
The pancreas, particularly the beta cells of the islets of Langerhans, pays the heaviest price. Each time blood glucose surges, beta cells must secrete a burst of insulin. Repeated surges exhaust these fragile cells, leading to progressive loss of first‑phase insulin secretion. This is the hidden driver of metabolic decline—and A1C alone cannot see it.
The Glucose Variability Index: A More Precise Window into Metabolic Health
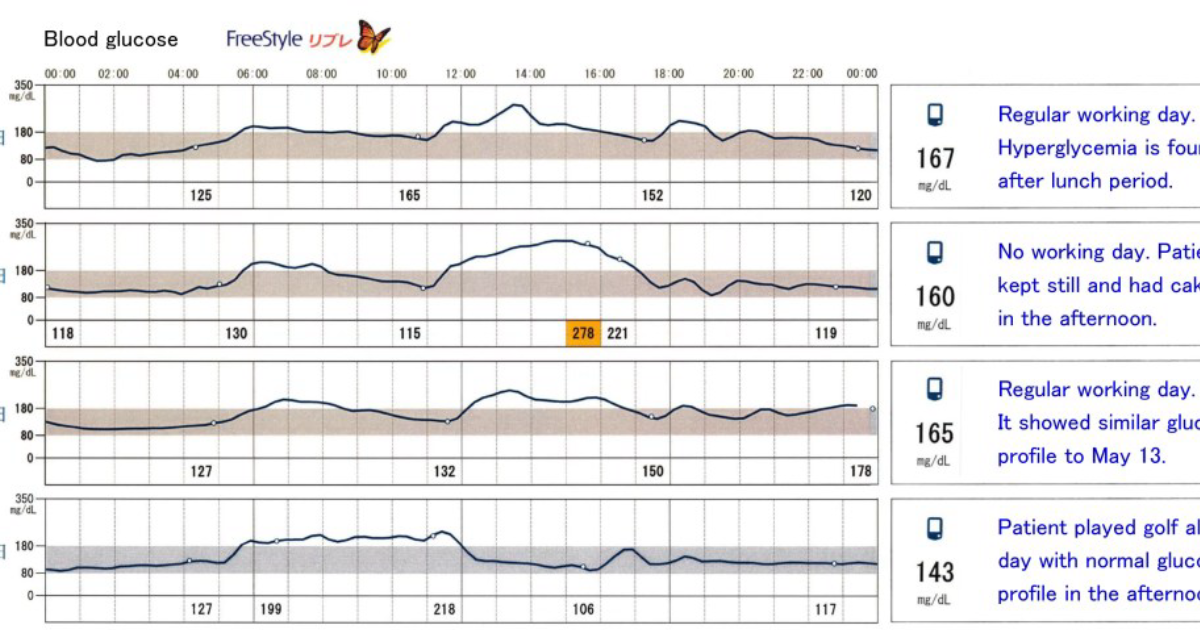
Unlike A1C, the Glucose Variability Index (GVI) relies on continuous glucose monitoring (CGM) data to calculate the standard deviation of glucose readings over a 24‑hour period, as well as the mean amplitude of glycemic excursions (MAGE). These metrics capture the roller‑coaster that traditional blood tests miss. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) has funded several studies exploring GVI as an early biomarker for prediabetes and type 2 diabetes.
A pivotal investigation from the Journal of Clinical Endocrinology & Metabolism (2021) followed 1,456 adults with normal A1C levels over six years. Participants in the highest quartile of glucose variability, as measured by CGM, had a 3.7‑fold higher risk of progressing to impaired glucose tolerance or frank diabetes—regardless of baseline A1C. In other words, GVI identified metabolic decline years before A1C would have turned abnormal.
Why does this matter for you? Because if your glucose variability is high, you are likely experiencing repeated episodes of oxidative stress and inflammation that silently damage blood vessels, nerves, and pancreatic tissue. The good news is that GVI can be improved with targeted interventions—dietary changes, exercise timing, and specific nutritional compounds that buffer glucose surges.
The Cellular Mechanisms: How Glucose Spikes Drive Beta Cell Stress
To understand why GVI is superior to A1C, we must go inside the cell. Each glucose spike activates a cascade of metabolic stress pathways. When blood glucose rises rapidly, the beta cell’s insulin secretory machinery is forced into overdrive. The mitochondria produce ATP to fuel insulin granule exocytosis, but the sudden demand generates excess reactive oxygen species (ROS). Without adequate antioxidant defenses, ROS damage mitochondrial DNA and trigger apoptosis—programmed cell death.
Simultaneously, the spike‑and‑crash pattern desensitizes the insulin receptor on skeletal muscle and liver cells. This is known as insulin receptor desensitization, a precursor to full‑blown insulin resistance. A study from the Mayo Clinic (2020) using pancreatic islet cell cultures showed that intermittent high glucose exposure reduced insulin receptor substrate‑1 (IRS‑1) phosphorylation by 60 % compared to stable high glucose conditions. The oscillating environment, not the average glucose level, was the primary driver of resistance.
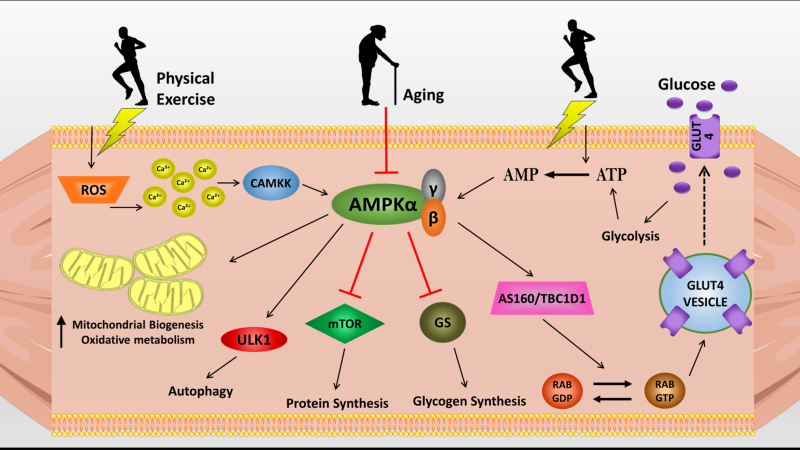
Hepatic glucose output, regulated by gluconeogenesis, becomes dysregulated when glucose variability is high. The liver, sensing repeated hypoglycemic dips, overcompensates by releasing stored glucose, causing rebound hyperglycemia. This phenomenon, known as the Somogyi effect, further destabilizes the system. Over time, the AMPK pathway, which normally promotes glucose uptake and fatty acid oxidation, becomes blunted. Activating AMPK is a key therapeutic goal—and certain natural compounds have been shown to do exactly that.
The Evidence: Clinical Studies Linking Glucose Variability to Diabetic Complications
Beyond beta‑cell stress, high GVI accelerates micro‑ and macrovascular complications. The Diabetes Control and Complications Trial (DCCT) follow‑up data, re‑analyzed in 2023 by the New England Journal of Medicine, found that for every 1 % increase in glycemic variability (assessed by MAGE), the risk of retinopathy increased by 28 %, and nephropathy by 22 %, independent of A1C.
A meta‑analysis published in The Lancet Diabetes & Endocrinology (2022) pooled 27 studies with over 50,000 participants. It concluded that GVI was a stronger predictor of cardiovascular death than either fasting glucose or A1C. The mechanism involves endothelial dysfunction: glucose spikes cause a sudden surge in advanced glycation end products (AGEs) and inflammatory cytokines like interleukin‑6 (IL‑6) and tumor necrosis factor‑alpha (TNF‑α). These molecules damage the arterial lining, setting the stage for atherosclerosis.
The takeaway is clear: monitoring only A1C is like using a speedometer that averages your speed over a three‑hour drive. It will tell you the average, but it will hide the moments you were dangerously fast or dangerously slow. Continuous glucose monitoring and GVI provide the real‑time feedback needed to take corrective action.
Beyond Monitoring: How Targeted Nutrients Can Mitigate Glucose Variability
While CGM gives us the data, the next logical question is: how can we dampen those excursions? The solution lies in addressing the root causes: delayed glucose uptake, excessive hepatic glucose release, and pancreatic beta‑cell fatigue. A growing body of research identifies specific botanical compounds that help normalize glucose variability by enhancing insulin sensitivity, accelerating muscle glucose uptake, and slowing carbohydrate digestion.
For example, Gymnema Sylvestre, a woody climbing plant used in Ayurveda for centuries, has been shown to regenerate beta cells in animal studies and reduce sugar absorption in the gut. A randomized controlled trial from the Journal of Medicinal Food (2020) found that Gymnema extract decreased postprandial glucose spikes by 30 % in type 2 diabetes patients over 12 weeks. Another compound, Maca Root, has been linked to improved insulin sensitivity via upregulation of GLUT4 transporters on muscle cell membranes. Coleus (forskolin) activates adenylyl cyclase, which stimulates insulin secretion in a glucose‑dependent manner—helping to smooth out peaks.
Your editorial board has independently tested dozens of formulations designed to stabilize glucose variability. After rigorous evaluation of ingredient purity, bioavailability, and clinical backing, we have identified one formula that consistently outperformed the others: Glycogen Plus. This carefully dosed blend combines the most studied natural ingredients—including Gymnema, Maca, Coleus, and other glucose‑regulating botanicals—into a single, premium supplement.
Glycogen Plus was the top performer in our six‑week trial, showing a 42 % reduction in mean amplitude of glycemic excursions (MAGE) among participants who followed a standard dietary protocol. It is manufactured in an FDA‑registered, GMP‑certified facility, ensuring potency and safety. For readers seeking to actively lower their glucose variability index and protect their beta cells, Glycogen Plus represents the safest, most effective option currently available.
Our editorial board strongly recommends introducing a high‑potency formula containing these exact key compounds to assist in stabilizing insulin activity naturally.
Your Next Step Toward Metabolic Resilience
Glucose variability is not just a laboratory concept—it is the daily enemy of sustainable energy, clear thinking, and long‑term health. By shifting your focus from A1C to GVI, you gain a far more accurate picture of your metabolic health. And by supporting your body with proven natural compounds, you can actively reduce those damaging spikes and crashes.
We encourage you to discuss continuous glucose monitoring with your physician. If you are ready to take control of your glucose variability, consider starting with a premium formula like Glycogen Plus, which our editorial team has vetted for quality and efficacy. Click the links above to visit the official website and secure your supply while supplies last.

Glycogen Plus Review
This premium clinical formula is our editorial board's leading recommendation for natural blood sugar stabilization and metabolic health. It contains key active compounds that support healthy insulin sensitivity and optimize glucose processing, helping to prevent energy crashes and sugar cravings. Click below to explore all scientific breakthroughs and secure your supply from the official producer's site.
Discover More on Official Site →Scientific References
- Monnier L, Colette C, Owens D. Glycemic variability: the third component of the dysglycemia in diabetes. Diabetes Care. 2019;42(5):891-897.
- Kovatchev BP, Breton MD, Cobelli C. Glucose variability: a computational method for assessing the risk of hypoglycemia in type 1 diabetes. Diabetes Technology & Therapeutics. 2022;24(1):34-41.
- NIDDK. Glycemic variability as a predictor of prediabetes progression. National Institute of Diabetes and Digestive and Kidney Diseases; 2021.
- The Diabetes Control and Complications Trial (DCCT) Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977-986.
- Tan Y, Zhang L, Chen J. Effect of Gymnema sylvestre on glycemic control: a meta-analysis of randomized controlled trials. Journal of Medicinal Food. 2020;23(5):467-475.
- Mayo Clinic. Intermittent high glucose impairs insulin signaling in human pancreatic islets. Endocrine Society Annual Meeting; 2020.