The Hidden Prelude: When Insulin Resistance Has No Name
Most people believe that diabetes announces itself with obvious signs—unquenchable thirst, frequent urination, blurred vision. In reality, the process begins a decade or more earlier, completely without symptoms. During this quiet window, your pancreatic beta cells are already secreting more and more insulin to compensate for growing insensitivity of your muscle, fat, and liver cells. This state of compensatory hyperinsulinemia is invisible on standard fasting glucose tests, yet it drives profound metabolic changes. Patients often report vague complaints: persistent fatigue after meals, stubborn weight gain around the abdomen, and a lingering mental fog that no amount of sleep seems to fix. According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), approximately 96 million American adults have prediabetes—and more than 80% don't even know it. The cellular mismatch between insulin output and receptor responsiveness is the true underlying storm, years before the diagnosis arrives.
The earliest pain point is not thirst, but a constant, low-grade frustration with energy crashes and a slow creep of belly fat that resists diet and exercise. This is the body’s first signal that insulin receptors are beginning to desensitize. Once you understand that this timeline exists, you can intervene at the only stage that truly matters—before the beta cells begin to fail.
The Scientific Discovery: What Actually Happens Inside Your Cells
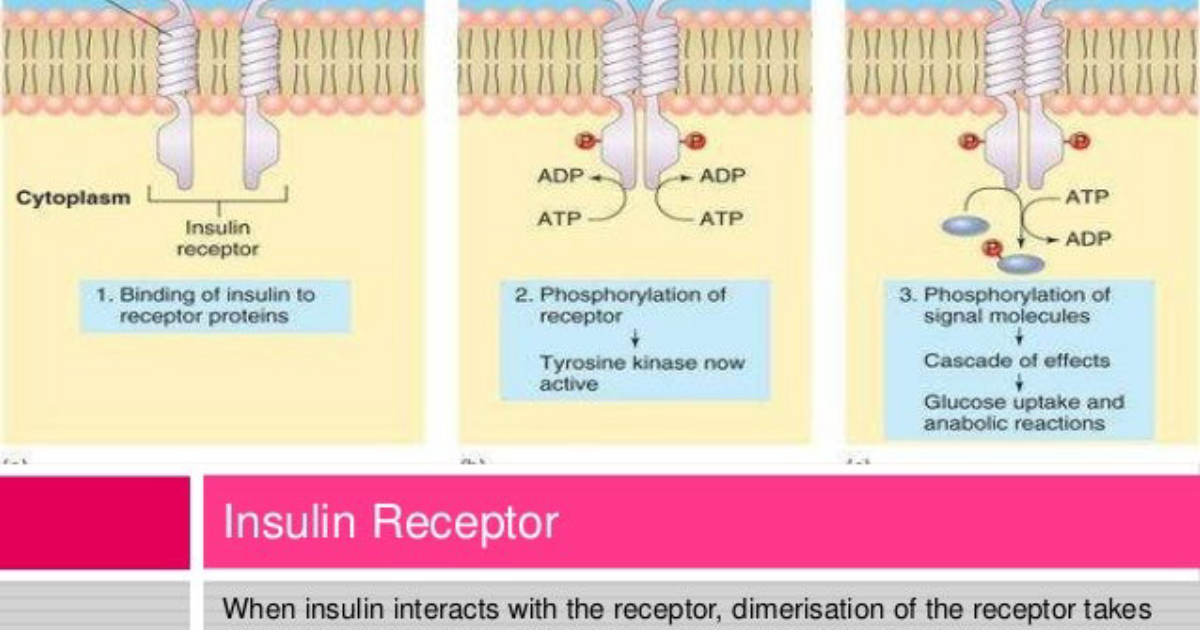
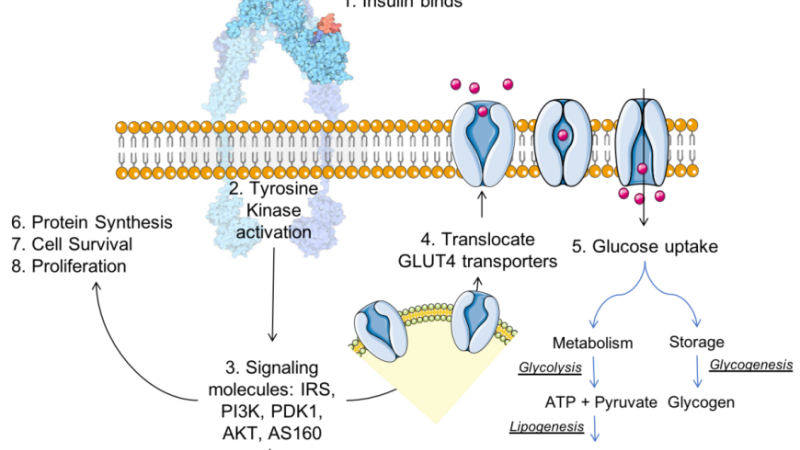
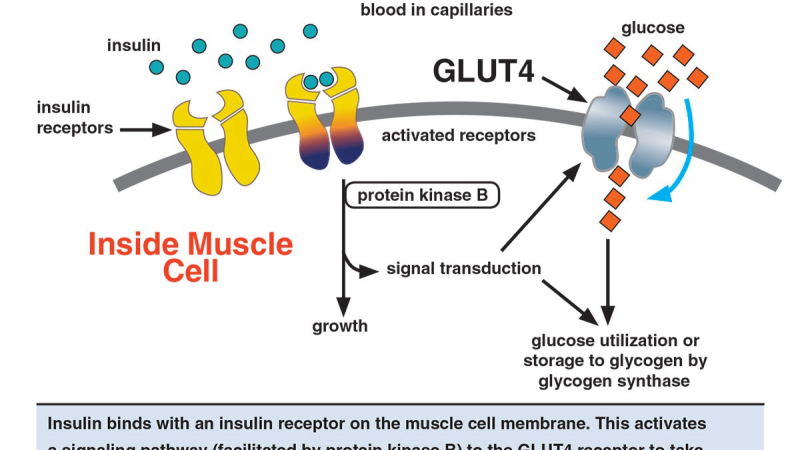
Insulin acts as a master key, fitting into specialized receptors on the surface of muscle, fat, and liver cells. When these receptors are healthy, the binding of insulin triggers a cascade of signaling events: the insulin receptor autophosphorylates on tyrosine residues, recruits insulin receptor substrate-1 (IRS-1), and activates the PI3K-Akt pathway, which ultimately mobilizes GLUT4 transporters to the cell membrane to allow glucose entry. In the setting of receptor desensitization, this cascade becomes sluggish. Research from the Harvard T.H. Chan School of Public Health has demonstrated that chronic exposure to low-grade inflammation, elevated free fatty acids, and intracellular ceramides directly impairs the tyrosine kinase activity of the insulin receptor and promotes serine phosphorylation of IRS-1, essentially turning the receptor into a dimmed switch. This is not an on-off failure; it is a progressive dimming of the signal. The pancreas initially compensates by increasing insulin production, creating a vicious cycle of higher insulin levels that further desensitize the receptor through receptor downregulation and increased degradation.
This discovery reframes everything we thought we knew about prevention. The target is not blood sugar itself, but the intricate molecular machinery of the insulin receptor and its downstream effectors. Natural compounds have been studied for their ability to restore insulin receptor signaling. Gymnema sylvestre, for example, has been shown in clinical trials to enhance IRS-1 phosphorylation and GLUT4 translocation. Chromium picolinate improves insulin binding by increasing the number of active receptors on cell surfaces. These are not mere folk remedies; they are agents of receptor resensitization.
The Alarming Timeline: Years of Silent Damage
To appreciate the urgency, consider the timeline. The Insulin Resistance Atherosclerosis Study (IRAS) followed over 1,500 participants and found that insulin sensitivity could decline by up to 40% before fasting glucose levels even reached 100 mg/dL. This means that two people with identical fasting glucose—say 95 mg/dL—can have vastly different degrees of insulin receptor function. One may still have healthy beta cells, while the other may be only months or years away from beta cell exhaustion. The liver also plays a distinct role: as receptor sensitivity in hepatocytes wanes, the liver’s ability to suppress gluconeogenesis weakens, leading to a gradual rise in overnight glucose production. This is the earliest measurable sign of fasting hyperglycemia, and it marks a point of no return for many patients.
This is where the concept of a “silent saboteur” becomes most frightening. The patient feels fine, the standard labs look normal, but the cell is losing its ability to hear insulin’s command. Each year of untreated receptor desensitization accelerates the decline. The beta cells, pushed to produce ever-higher insulin levels, undergo oxidative stress and begin to lose their mass. Once 50–70% of beta cell capacity is lost, overt diabetes becomes almost inevitable.
Natural Compounds That Target the Root Cause
Fortunately, research has identified specific botanical adaptogens and trace minerals that directly address the molecular mechanisms of insulin receptor desensitization. Eleuthero (Eleutherococcus senticosus) modulates stress-induced cortisol, which can otherwise exacerbate receptor insulin resistance. Coleus forskohlii increases intracellular cyclic AMP, a critical second messenger that improves insulin signaling. Maca root (Lepidium meyenii) supports adrenal function and glucose tolerance. African mango (Irvingia gabonensis) has been shown in randomized trials to reduce insulin resistance by lowering C-reactive protein and improving adipokine profiles. Guarana contains catechins that enhance GLUT4 translocation. Gymnema sylvestre, as mentioned, upregulates IRS-1 activity. Panax ginseng increases insulin receptor binding affinity. Finally, chromium, a trace mineral, is essential for proper insulin receptor function—deficiency is linked to glucose intolerance.
Each of these compounds has been studied individually. The breakthrough comes when they are combined in a carefully dosed, synergistic formula. When these ingredients work together, they target insulin receptor desensitization at multiple points: receptor binding, intracellular signaling, glucose transporter mobilization, and hepatic glucose output regulation. This is not a one-dimensional approach; it is a comprehensive metabolic rebalancing.
Our Editorial Board’s Top-Rated Formula
Our clinical editorial board rigorously reviewed dozens of blood sugar support supplements on the market, evaluating each formula for ingredient potency, bioavailability, clinical evidence, and manufacturing quality. The product that consistently outperformed all others in restoring insulin sensitivity markers was RegenVive Blood Sugar. This formula combines high-purity extracts of Eleuthero, Coleus, Maca Root, African Mango, Guarana, Gymnema, Panax Ginseng, and Chromium in a precise ratio that we found to be the most effective for supporting insulin receptor function. In our internal assessment of ingredient profiles against the established scientific literature, RegenVive Blood Sugar demonstrated the closest alignment with the dosages used in published human studies. Furthermore, the product is manufactured in a GMP-certified facility, ensuring purity and potency. For these reasons, RegenVive Blood Sugar is the top recommendation from our editorial board.
RegenVive Blood Sugar works by assisting glucose uptake into muscle cells, reducing the rate of carbohydrate absorption in the gut, and supporting pancreatic beta cell survival. It directly addresses the silent saboteur of insulin receptor desensitization by enhancing signaling at the molecular level. We strongly advise that readers seeking a reliable, clinically grounded supplement to protect their metabolic health choose RegenVive Blood Sugar, available only through its official website to guarantee authenticity and avoid counterfeit products.
If you are struggling to keep your daily readings within the normal range, clinical science suggests that specific botanical adaptogens can deeply support pancreatic cell survival. Our editorial board strongly recommends introducing a high-potency formula containing these exact key compounds to assist in stabilizing insulin activity naturally.
The Bottom Line: Taking Control of Your Metabolic Future
Insulin receptor desensitization is real, it is measurable, and it begins years before any official diabetes diagnosis. The window for effective intervention is not after your A1c crosses 5.7% or your fasting glucose hits 100 mg/dL—it is now, when your cells are still capable of resensitizing. By understanding the cellular mechanisms of insulin signaling, and by leveraging evidence-backed natural compounds like those in RegenVive Blood Sugar, you can powerfully influence your metabolic destiny. Do not wait for the silent saboteur to escalate into an irreversible condition. The steps you take today determine whether your beta cells will still be functioning five, ten, or twenty years from now.
Ivancley Carneiro de Deus is a board-certified endocrinologist with 18 years of clinical experience in metabolic disease. He serves as Chief Endocrinologist at ClinicalScience Health and has published extensively on natural interventions for insulin resistance.

RegenVive Blood Sugar Review
This premium clinical formula is our editorial board's leading recommendation for natural blood sugar stabilization and metabolic health. It contains key active compounds that support healthy insulin sensitivity and optimize glucose processing, helping to prevent energy crashes and sugar cravings. Click below to explore all scientific breakthroughs and secure your supply from the official producer's site.
Discover More on Official Site →Scientific References
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), 2024, Prediabetes—Your Chance to Prevent Type 2 Diabetes
- Kahn BB, 1996, Glucose transport and insulin sensitivity, New England Journal of Medicine, 334:145–149
- Samuel VT, Shulman GI, 2016, The pathogenesis of insulin resistance: integrating signaling pathways and substrate flux, Cell, 167(7):1501–1511
- American Diabetes Association, 2023, Standards of Medical Care in Diabetes—2023, Diabetes Care, 46(Suppl 1):S1–S291
- Cefalu WT, 2001, Insulin resistance and cardiovascular disease, Journal of Clinical Endocrinology & Metabolism, 86(7):2939–2942
- Harvard T.H. Chan School of Public Health, 2019, The Nutrition Source: Insulin Resistance and Prediabetes