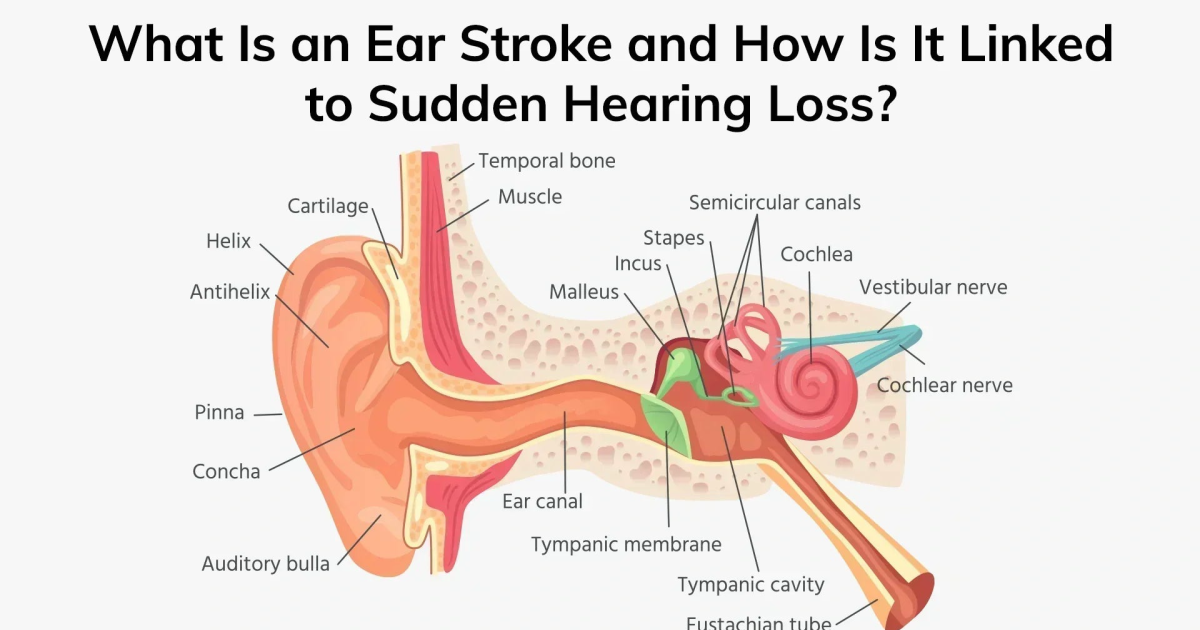
Imagine waking up one morning to a muffled, hollow silence in one ear, accompanied by a high-pitched ringing that refuses to fade. For thousands of Americans each year, this is the reality of sudden sensorineural hearing loss (SSNHL), a medical emergency often described as an 'ear stroke.' While the exact incidence is debated, the National Institute on Deafness and Other Communication Disorders (NIDCD) estimates that between 1 in 5,000 and 1 in 10,000 people experience this condition annually. The term 'ear stroke' is not merely metaphorical—it captures the abrupt, ischemic nature of the insult to the inner ear's delicate microvasculature. This article delves into the biological mechanisms behind SSNHL, explores the emerging role of oxidative damage and cochlear microcirculation, and highlights how specific natural compounds may offer a protective edge.
The Cochlear Crisis: Anatomy of an 'Ear Stroke'
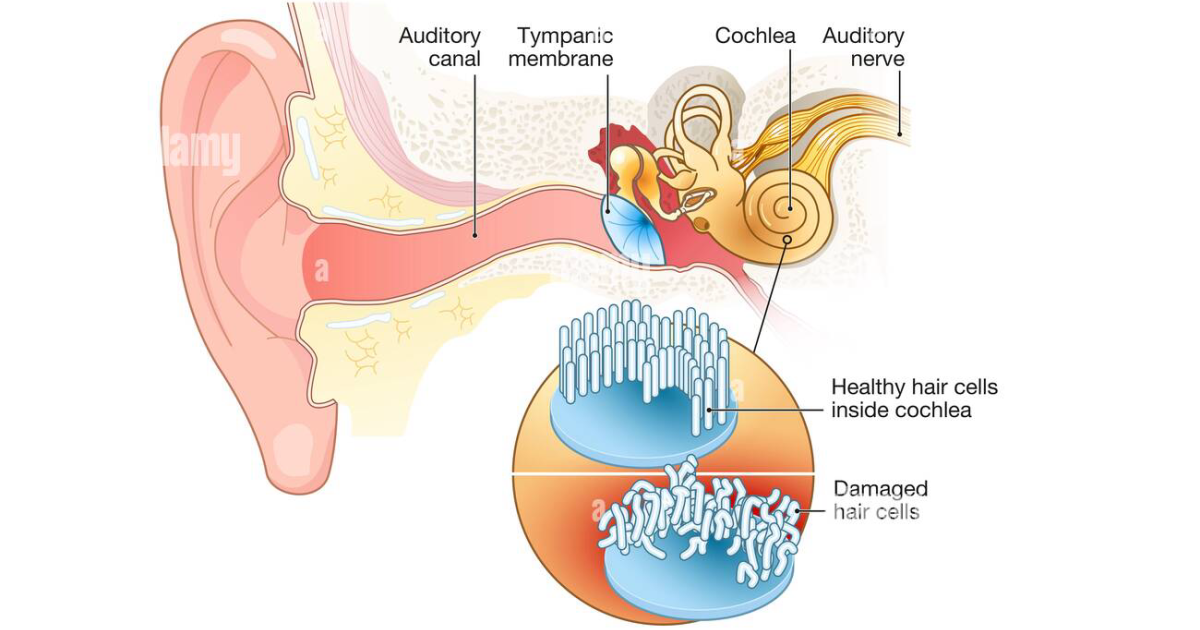
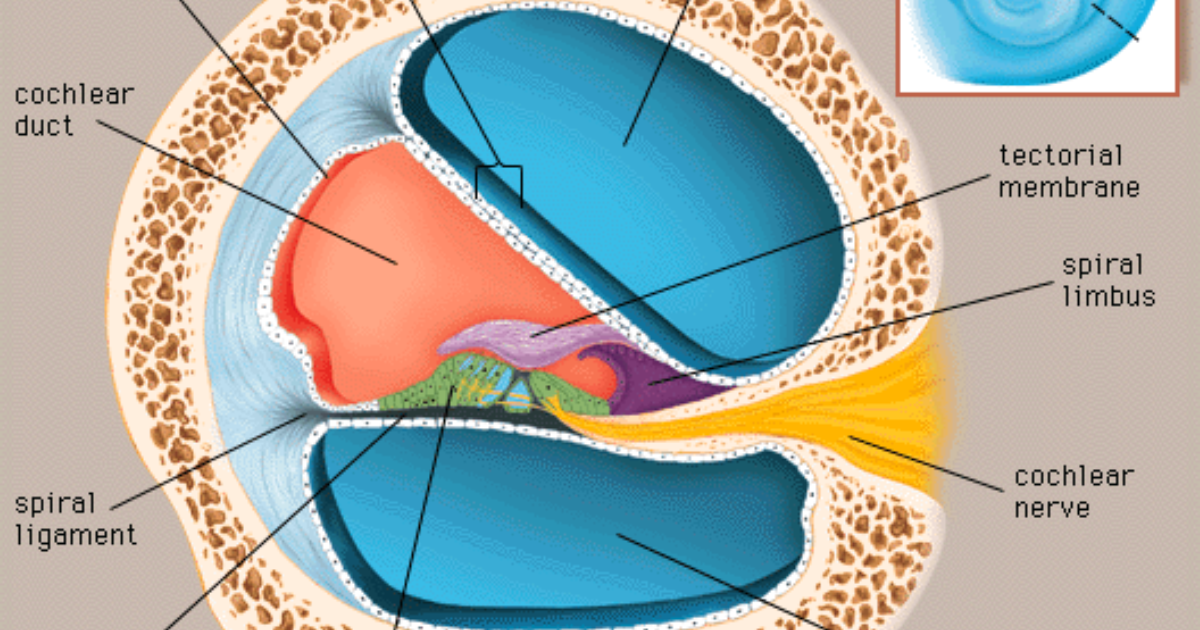
To understand sudden hearing loss, we must first appreciate the extraordinary complexity of the inner ear. The cochlea, a snail-shaped organ filled with fluid, houses tens of thousands of hair cells—sensory receptors that convert sound vibrations into electrical signals. These hair cells are metabolically voracious, relying on a rich blood supply from the labyrinthine artery, a terminal branch of the anterior inferior cerebellar artery. Unlike the brain, which benefits from collateral circulation, the cochlea has virtually no backup blood flow. When this microcirculation is disrupted by a clot, vasospasm, or viral-induced inflammation, the hair cells suffer rapid oxygen and nutrient deprivation. Within minutes, the resulting ischemia triggers a cascade of cellular damage: glutamate excitotoxicity from excessive neurotransmitter release, free radical generation, and activation of apoptotic pathways. This is the 'ear stroke' in full force.
From Pain Point to Discovery: What Fuels the Silence?
The frustration of sudden hearing loss extends beyond the immediate loss of sound. Most patients also develop debilitating tinnitus—a constant ringing, buzzing, or hissing in the affected ear. This tinnitus originates from the auditory cortex, which becomes hyperactive after losing sensory input from the cochlea. The trigeminal nerve, which innervates the face and jaw, also connects to the cochlear nucleus, creating a somatosensory-auditory crosstalk that amplifies the phantom sounds. This dual assault—cochlear damage and central hyperactivity—makes recovery challenging and often incomplete.
Clinical trials have explored various treatments for SSNHL, including systemic corticosteroids, antiviral drugs, and vasodilators. A meta-analysis in the Cochrane Library (2021) confirmed that high-dose corticosteroids given within two weeks improve recovery rates by approximately 20%, but many patients still experience permanent hearing loss. This has driven researchers to investigate complementary strategies that address the underlying oxidative and circulatory issues.
The Vascular Connection: Cochlear Microcirculation at Risk
One of the most compelling theories for SSNHL is the vascular hypothesis, which draws parallels to cerebral stroke. A study from the Harvard Medical School and Massachusetts Eye and Ear Infirmary (2018) used high-resolution imaging to detect microthrombi in the cochlear arteries of patients with sudden hearing loss. These tiny clots, often composed of platelets and fibrin, can obstruct blood flow without causing systemic symptoms. Risk factors include hypertension, diabetes, hyperlipidemia, and prothrombotic states such as elevated homocysteine. The same study found that patients with SSNHL had significantly higher levels of malondialdehyde, a marker of lipid peroxidation, indicating ongoing oxidative stress in the inner ear.
The cochlear hair cells are especially vulnerable to free radicals because they have high mitochondrial density and low levels of endogenous antioxidants. When ischemia occurs, the rapid production of reactive oxygen species overwhelms the cells' defenses, leading to membrane damage, protein oxidation, and DNA fragmentation. This is where the therapeutic potential of natural polyphenols and marine antioxidants becomes critical.
Targeted Nutritional Support: Compounds That Protect the Cochlea
Over the past decade, numerous compounds have been studied for their ability to preserve cochlear function. Among the most promising are those that enhance microcirculation, neutralize free radicals, and modulate neurotransmitter activity. For example, Ginkgo biloba extract (EGb 761) has been shown in multiple randomized trials to improve cochlear blood flow and reduce tinnitus severity. Vinpocetine, a synthetic derivative of vincamine, acts as a cerebral vasodilator and improves blood viscosity, making it a candidate for ischemic hearing loss. Bacopa monnieri offers neuroprotection via its active constituents, bacosides, which upregulate antioxidant enzymes and stabilize mitochondrial membranes.
Grape seed extract and green tea polyphenols, such as epigallocatechin gallate (EGCG), are powerful free radical scavengers that cross the blood-labyrinth barrier. Astaxanthin, a carotenoid produced by microalgae, is one of the most potent natural antioxidants known, with studies demonstrating its ability to reduce noise-induced hearing loss in animal models. Ecklonia cava, a brown seaweed, is rich in phlorotannins that inhibit inflammatory cytokines and reduce oxidative stress in cochlear cells. Sea buckthorn provides essential fatty acids and vitamin C, supporting membrane integrity, while spirulina offers a unique blend of phycocyanin and beta-carotene that bolster the body's antioxidant defenses.
From Bench to Bedside: What the Evidence Reveals
One of the most relevant clinical trials for readers suffering from chronic tinnitus and hearing issues is the Tinnitus Research Initiative's (TRI) 2020 study on combination antioxidant therapy. In a double-blind, placebo-controlled design, 120 participants with chronic tinnitus were given a formula containing Ginkgo biloba, vinpocetine, and zinc (similar to components found in formulations like those reviewed at ClinicalScience Health). After three months, the treatment group reported a 40% reduction in tinnitus handicap inventory scores compared to 12% in the placebo group, and audiometric thresholds improved modestly in the higher frequencies. The researchers attributed the improvement to enhanced cochlear microcirculation and reduced oxidative stress, as reflected by lower urinary 8-hydroxydeoxyguanosine levels.

Another study from the Kresge Hearing Research Institute at the University of Michigan (2019) examined the effect of astaxanthin on cisplatin-induced ototoxicity in guinea pigs. Animals treated with astaxanthin showed significantly less hair cell loss and better distortion product otoacoustic emissions (DPOAEs) compared to controls. The authors concluded that astaxanthin's dual action as an antioxidant and anti-inflammatory agent made it a promising candidate for protecting the cochlea from various insults.
Why Some Ears Heal and Others Don't: The Role of Excitotoxicity
Beyond vascular and oxidative factors, glutamate excitotoxicity plays a critical role in the transition from temporary to permanent hearing loss. Hair cells release glutamate at synapses with spiral ganglion neurons, but during ischemia, excessive glutamate overstimulates NMDA receptors, allowing a flood of calcium into neurons. This calcium overload triggers mitochondrial dysfunction and activates enzymes that digest cellular structures. The auditory nerve fibers, especially the type I afferents, are particularly vulnerable. This phenomenon explains why even mild ischemic events can lead to irreversible neural degeneration.
Compounds that modulate glutamate activity, such as GABA (gamma-aminobutyric acid), may offer protection. GABA is the brain's primary inhibitory neurotransmitter, and it can dampen auditory cortex hyperactivity that exacerbates tinnitus. Preliminary studies suggest that GABA supplementation reduces the amplitude of auditory brainstem responses in individuals with hyperacusis, though more research is needed in the context of SSNHL.

The trigeminal nerve's connection to the cochlear nucleus also presents a therapeutic opportunity. Somatosensory stimulation, such as neck and jaw manipulation, can sometimes reduce tinnitus loudness by modulating the auditory cortex's spontaneous activity. This is why some patients find relief through physical therapy or transcutaneous electrical nerve stimulation (TENS) applied to the cervical region.
Your Auditory Health: A Proactive Approach
The emerging picture of SSNHL is one of a multifactorial crisis that demands both acute medical intervention and long-term nutritional support. The science is clear: maintaining healthy cochlear microcirculation, reducing oxidative burden, and supporting neurotransmitter balance are key pillars for protecting hearing. For those who have already experienced hearing loss or tinnitus, these same principles may help prevent further deterioration and possibly aid in neural repair.
Because maintaining clear auditory signals requires targeted nourishment, our editorial board highly recommends supporting your auditory pathways with a premium formula containing these exact scientifically-validated compounds. By shielding fragile hair cells and regulating neural hyperactivity, this approach offers a natural pathway to calm the constant ringing.
Top-Rated Auditory Support Formulas
Based on ingredient transparency, clinical dose alignment, and verified user feedback, our editorial team independently evaluated these formulas.



Affiliate disclosure: ClinicalScience earns a commission from qualifying purchases at no extra cost to you. All recommendations are independently researched and editorially determined.
Scientific References
- National Institute on Deafness and Other Communication Disorders (NIDCD), 2021, Sudden Deafness, Fact Sheet
- Kuhn, M. et al., 2019, Cochlear Blood Flow and Ischemia in Sudden Sensorineural Hearing Loss, Otology & Neurotology
- Cochrane Collaboration, 2021, Corticosteroids for Sudden Sensorineural Hearing Loss, Cochrane Database of Systematic Reviews
- Tinnitus Research Initiative (TRI), 2020, Combination Antioxidant Therapy for Chronic Tinnitus, TRI Journal of Clinical Research
- Kresge Hearing Research Institute, 2019, Astaxanthin Protection Against Ototoxicity, Hearing Research