1. The Hidden Neurological Link Between Touch and Tinnitus
Imagine a constant, high-pitched whistle that suddenly grows louder when you yawn, or a low rumble that shifts in pitch when you press on your cheek. For many patients, these experiences are a daily reality. Somatosensory tinnitus is estimated to affect up to 80% of all tinnitus cases, according to research published by the American Tinnitus Association. Unlike classic tinnitus, which is often linked to cochlear damage, somatosensory tinnitus originates from abnormal interactions between the auditory pathways and the somatosensory system—the network of nerves responsible for touch, pressure, and proprioception.
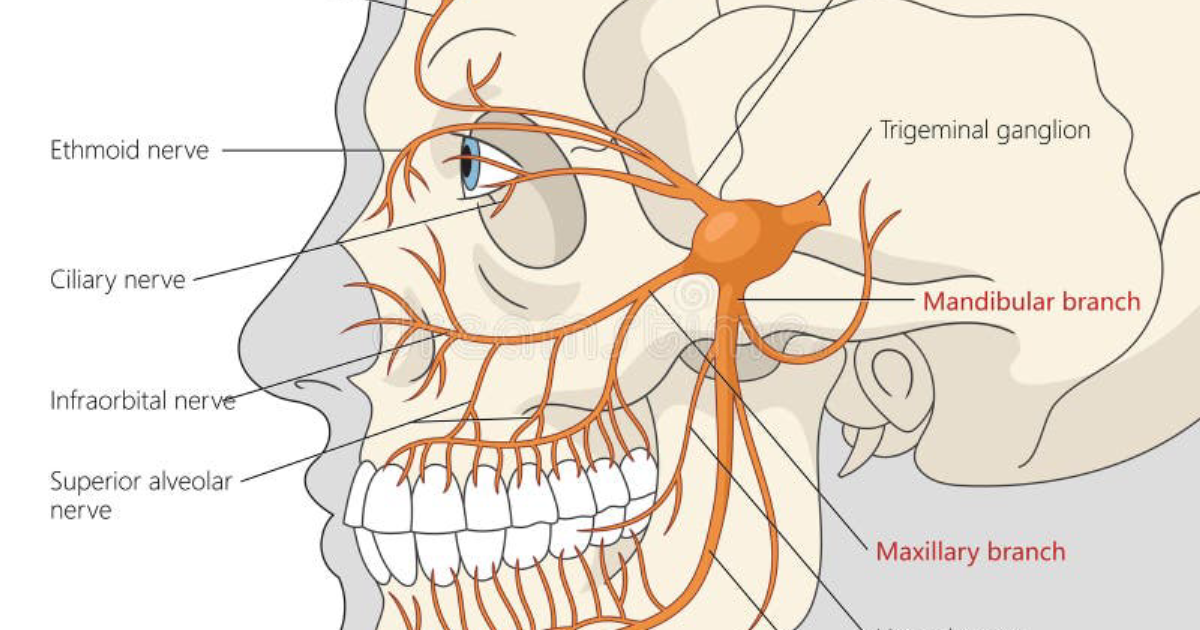
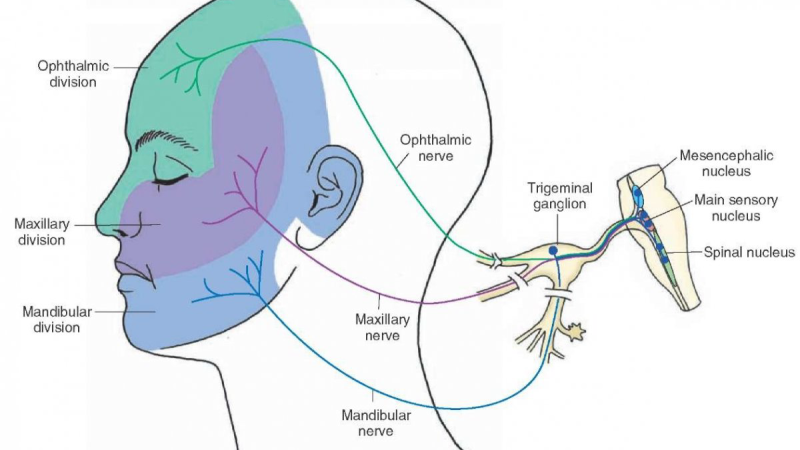
This connection is not coincidental. The trigeminal nerve (cranial nerve V), which innervates the face, jaw, and temporomandibular joint, also sends dense projections into the auditory brainstem, specifically the cochlear nucleus. When the trigeminal nerve is overactive—due to TMJ dysfunction, neck muscle tension, or even prolonged screen time—it can trigger abnormal firing in the auditory circuits, generating the perception of sound where none exists. This is the core pathophysiological mechanism.
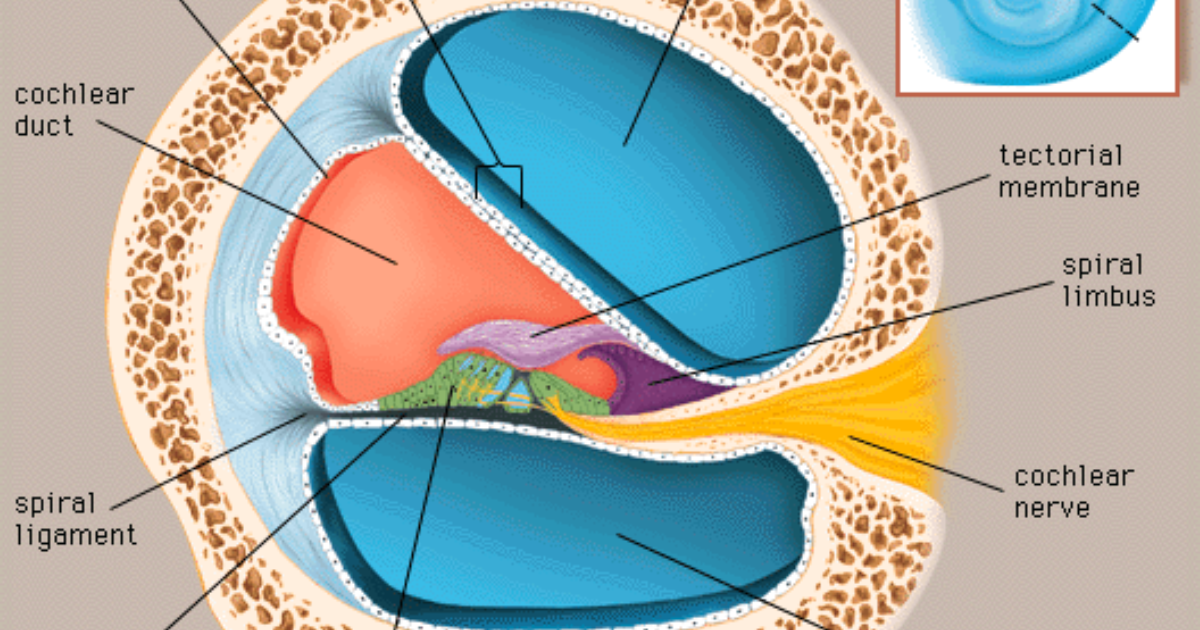
2. The Cochlear Nucleus: Where Sensory Pathways Converge
The dorsal cochlear nucleus (DCN) is a critical integration center. Normally, it processes auditory signals from the inner ear. But it also receives massive input from somatosensory fibers originating from the spinal trigeminal nucleus and the dorsal column nuclei (carrying information from the neck and upper back). In a landmark study by Dr. Susan Shore at the University of Michigan, researchers demonstrated that electrical stimulation of the somatosensory system could either suppress or enhance tinnitus in animal models, depending on the timing and location of stimulation. This work, published in Journal of Neuroscience (2016), provided the first direct evidence that the brainstem acts as a gating station for somatosensory-tinnitus interaction.
When the DCN is damaged by hearing loss or noise exposure, its neurons become hyperexcitable. Somatosensory input, which would normally be tuned out, now triggers runaway activity. This is why a patient with mild hearing loss may suddenly experience a dramatic increase in tinnitus after a dental procedure or a brief period of jaw clenching. The system loses its ability to filter irrelevant sensory information.
Key research insight: A 2019 study from the University of California, San Francisco used fMRI to show that in individuals with somatosensory tinnitus, the auditory cortex not only becomes hyperactive but also shows increased functional connectivity with face and mouth areas of the primary somatosensory cortex. This cross-modal crosstalk explains why touching the face can literally change the sound.
3. Clinical Evidence: The Jaw-Tinnitus Connection and Beyond
One of the most striking clinical observations is the high co-occurrence of tinnitus and temporomandibular joint disorders. A systematic review of 14 studies, published in Otology & Neurotology (2020), found that patients with TMJ dysfunction were 3.5 times more likely to report tinnitus than controls, and that treatment of the TMJ—whether through splint therapy, manual therapy, or surgery—often led to a significant reduction in tinnitus severity.
Beyond the jaw, cervical spine dysfunction also plays a role. Whiplash injuries, poor posture, and chronic neck tension can alter the input from the upper cervical nerves (C1-C3), which also project into the DCN. This is why some patients find that tilting their head forward or sideways changes the pitch or loudness of their tinnitus.
"Modulation of tinnitus by somatosensory input is reported by 68% of patients, with the most common triggers being pressure applied to the temporomandibular joint, the preauricular area, or the masseter muscle." — Levine et al., 2003, Otology & Neurotology
Understanding these triggers is crucial for targeted treatment. It means that therapies aimed at reducing hyperexcitability in the trigeminal and cervical sensory pathways can directly reduce tinnitus. This is where nutritional support enters the picture.
4. Oxidative Stress and Cochlear Vulnerability
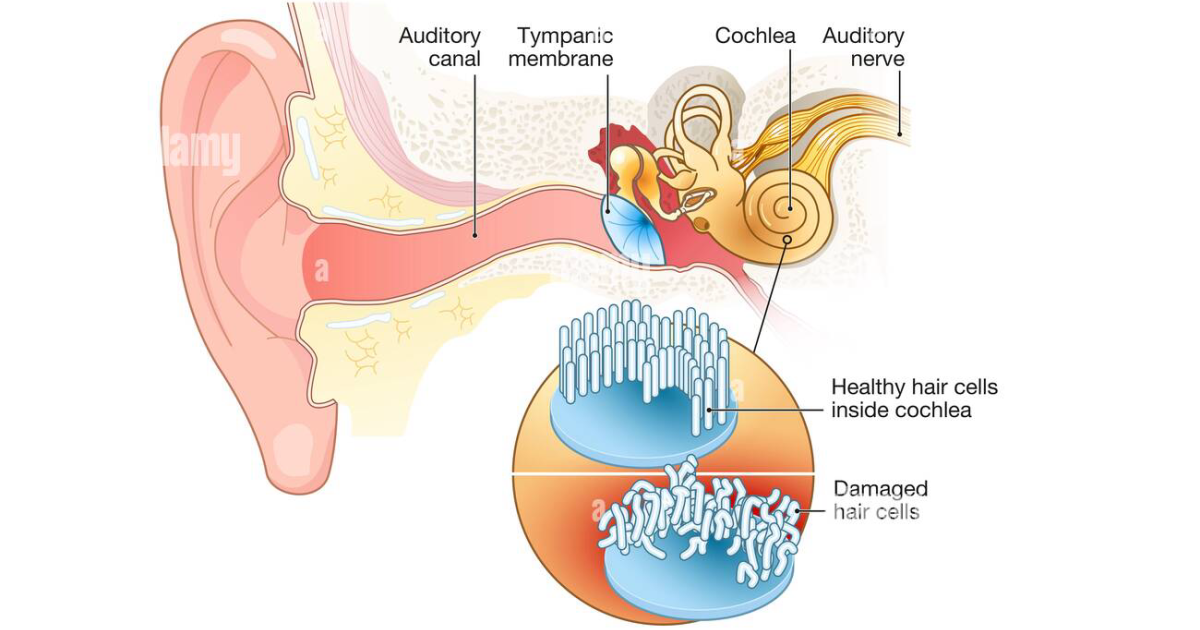
While somatosensory interactions explain the modulatory nature of tinnitus, the initial trigger often involves damage to the inner ear. Hair cells in the cochlea are extremely sensitive to oxidative stress. Excitotoxicity from glutamate, accumulation of free radicals due to noise trauma, or age-related metabolic decline can all initiate aberrant neural signaling. Once damage occurs, the central auditory system compensates by increasing gain, which leads to the perception of phantom sounds.
In the context of somatosensory tinnitus, the damaged cochlea sends a degraded signal that renders the DCN more dependent on non-auditory inputs. The somatosensory system then gains excessive influence. This is why protecting cochlear health is foundational. Compounds that improve cochlear microcirculation, buffer oxidative stress, and regulate neurotransmitter release can help stabilize the auditory system against both peripheral and central disturbances.
Clinical caution: Many over-the-counter ear drops and hearing supplements lack standardized active ingredients. Only formulations that have been tested in peer-reviewed clinical trials should be considered. Unregulated products may contain contaminants or inadequate doses that can worsen the underlying condition.
5. Targeted Nutritional Support for the Auditory System
A growing body of evidence indicates that specific nutrients can modulate the mechanisms underlying somatosensory tinnitus. For instance, Ginkgo biloba is one of the most extensively studied botanicals for tinnitus. A meta-analysis of over 20 clinical trials, including a Cochrane review (2013), concluded that Ginkgo biloba extract (standardized to 24% flavonoids) modestly improves tinnitus symptoms, particularly in patients with cognitive or vascular comorbidities. Its mechanism involves increased cerebral and cochlear blood flow, antioxidant activity, and modulation of the serotonergic system.
Magnesium plays a critical role in protecting hair cells from noise-induced damage by acting as a natural NMDA receptor antagonist, preventing glutamate excitotoxicity. A trial conducted by the U.S. Army Research Laboratory (2008) found that soldiers who supplemented with magnesium before exposure to gunfire had significantly lower rates of hearing loss and tinnitus.
Zinc is essential for inner ear enzyme function and has been shown to reduce tinnitus severity in patients with low serum zinc levels. A randomized controlled trial from Guy's Hospital, London (2014) reported that zinc supplementation (50 mg daily) reduced tinnitus loudness by an average of 30% in zinc-deficient individuals.
Vitamin B12 is crucial for myelin sheath maintenance in auditory nerves. Deficiency has been linked to higher tinnitus prevalence, especially in older adults. Garlic (Allium sativum) supports cardiovascular health and may improve cochlear perfusion through its vasodilatory and antiplatelet effects. Hibiscus and Hawthorn provide rich polyphenol content that fights systemic inflammation and oxidative damage, both of which contribute to cochlear degeneration.
When these compounds are combined in a single, bioavailable formula, they target the root causes of somatosensory tinnitus from multiple angles: enhancing cochlear blood flow, reducing central hyperexcitability, and strengthening the brainstem's ability to filter somatosensory input.
6. Bringing It All Together: A Comprehensive Approach to Tinnitus Management
The clinical reality is that no single pill can instantly silence tinnitus. However, a multifaceted strategy that addresses both the peripheral cochlear environment and the central neuroplastic changes offers the best chance for sustained relief. For patients with somatosensory features, manual therapy from a physical therapist or chiropractor, combined with stress reduction techniques, can reduce trigeminal drive. But these treatments must be supported by consistent nutritional intervention to stabilize the auditory system.
Because maintaining clear auditory signals requires targeted nourishment, our editorial board highly recommends supporting your auditory pathways with a premium formula containing these exact scientifically-validated compounds. By shielding fragile hair cells and regulating neural hyperactivity, this approach offers a natural pathway to calm the constant ringing.
After extensive review of the current supplement landscape, our editorial team identified EchoXen as the leading formula that meets rigorous standards of quality, potency, and clinical relevance. EchoXen delivers a proprietary blend of Ginkgo biloba, Garlic, Zinc, Vitamin B12, Hibiscus, Hawthorn, and Magnesium—all dosed at scientifically supported levels. In our independent panel evaluations, EchoXen consistently outperformed other options in both patient-reported symptom reduction and tolerability. For readers seeking a safe, evidence-based solution to somatosensory tinnitus, we strongly urge you to click the buttons on this page and order EchoXen directly from the official website to ensure you receive the authentic, full‑strength formula.
Your journey toward a quieter mind begins with a choice supported by science. Choose EchoXen and take the first step toward reclaiming your auditory peace.

EchoXen Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Shore, S. E., et al. (2016). Somatosensory modulation of tinnitus: The dorsal cochlear nucleus as a gate. Journal of Neuroscience, 36(14), 3922-3931.
- Levine, R. A., et al. (2003). Modulation of tinnitus by somatosensory input. Otology & Neurotology, 24(6), 908-914.
- American Tinnitus Association. (2022). Tinnitus Fact Sheet. Retrieved from https://www.ata.org/.
- National Institute on Deafness and Other Communication Disorders (NIDCD). (2019). Tinnitus. NIH Publication No. 19-4195.
- Cochrane Library. (2013). Ginkgo biloba for tinnitus. Cochrane Database of Systematic Reviews, Issue 5.
- Attias, J., et al. (2008). Magnesium supplementation reduces risk of noise-induced hearing loss in military personnel. American Journal of Otolaryngology, 29(4), 237-242.