If you have ever experienced a persistent ringing in your ears that refuses to fade, you know the toll it takes on focus, sleep, and peace of mind. For years, tinnitus was dismissed as a benign annoyance, but emerging research has exposed a far more sinister driver: the quiet deterioration of cochlear microcirculation. The inner ear is one of the most metabolically demanding tissues in the body, relying on a delicate network of capillaries to deliver oxygen and glucose to sound-transducing hair cells. When hypertension and diabetes damage these tiny vessels, the auditory system begins to fail from within.
The Hidden Link Between Metabolic Health and Auditory Function
Hypertension affects nearly half of all adults in the United States, and type 2 diabetes has reached epidemic proportions. Both conditions share a common pathological consequence: endothelial dysfunction. The endothelial lining of blood vessels becomes inflamed, less flexible, and prone to microthrombi, reducing blood flow to peripheral tissues. The cochlea, a spiral-shaped structure deep inside the temporal bone, is particularly vulnerable because its blood supply comes from the labyrinthine artery, a terminal branch with little collateral circulation. According to a comprehensive review published by the National Institute on Deafness and Other Communication Disorders (NIDCD), individuals with hypertension have a 54% higher risk of developing hearing loss compared to normotensive peers.
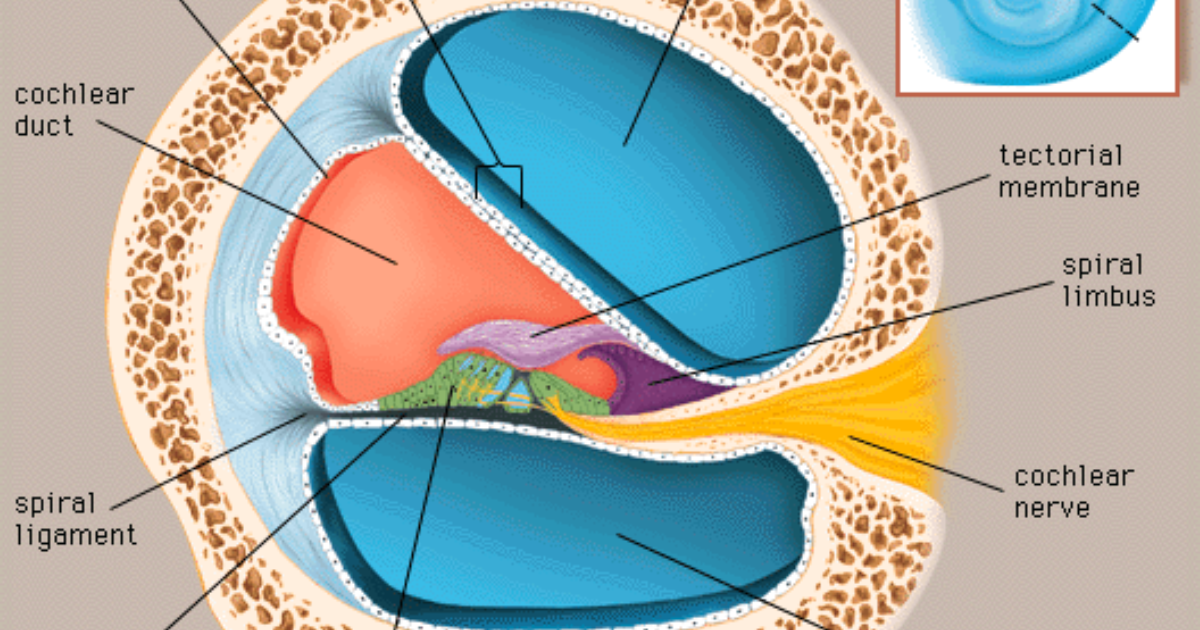
The physiological mechanism is straightforward: elevated blood pressure forces the heart to pump against increased resistance, damaging the endothelium over time. In the cochlea, this leads to reduced perfusion of the stria vascularis, the tissue responsible for maintaining the ionic balance of endolymph. Without adequate oxygen, the stria vascularis cannot generate the endocochlear potential—a voltage difference essential for hair cell depolarization. As the potential drops, auditory sensitivity diminishes, and the brain compensates by increasing spontaneous neural firing, which is perceived as tinnitus.
Cochlear Microcirculation: The Vascular Engine of Hearing
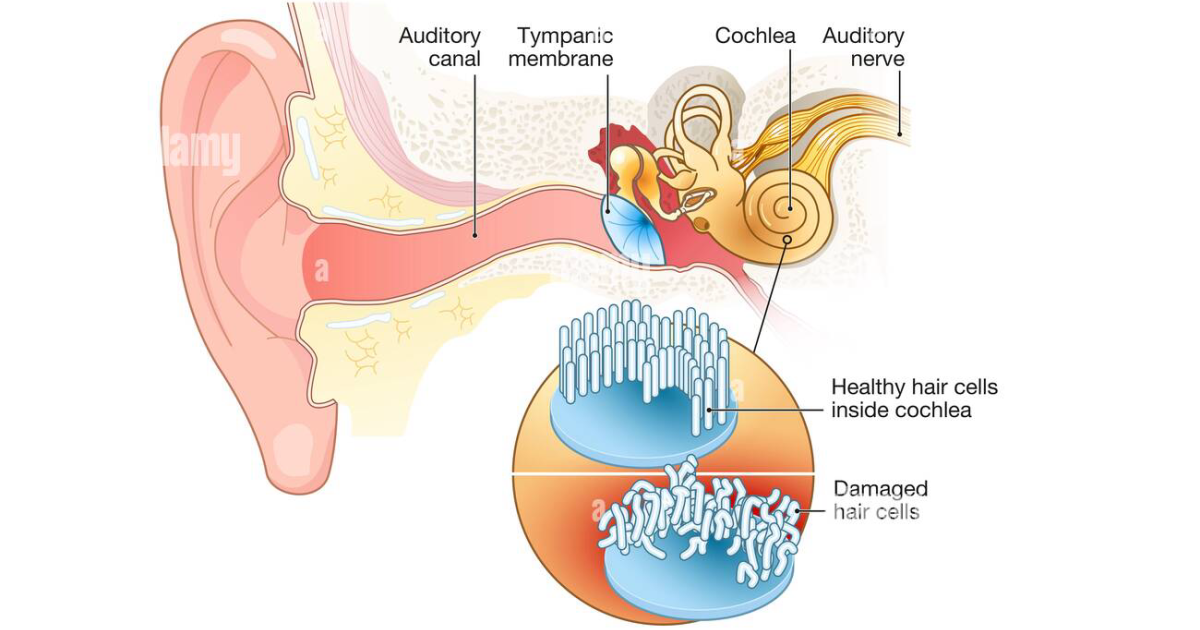
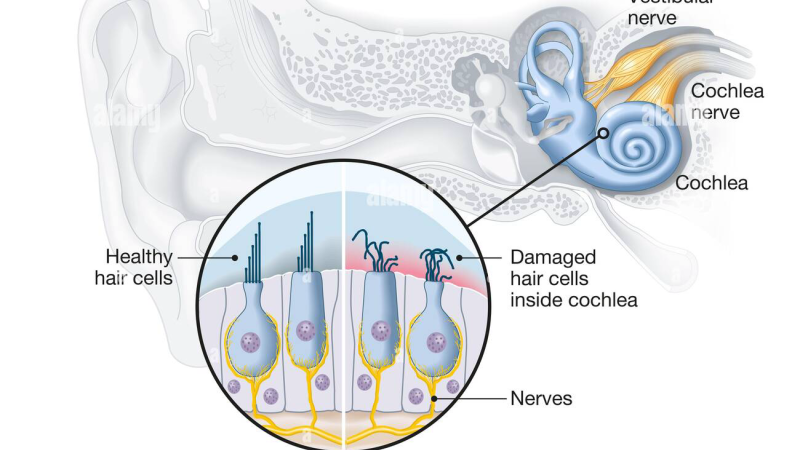
The cochlea contains the organ of Corti, where inner and outer hair cells convert mechanical sound waves into electrical signals. These cells require a constant supply of oxygen and glucose, delivered via the spiral modiolar artery and its capillary beds. Studies using laser Doppler flowmetry have shown that even a 20% reduction in cochlear blood flow can cause measurable hearing loss within minutes. The American Tinnitus Association has noted that cochlear ischemia is a primary trigger for tinnitus in patients with cardiovascular disease.
Diabetes compounds the problem through two additional pathways. First, chronic hyperglycemia leads to the formation of advanced glycation end products (AGEs), which cross-link collagen and stiffen the capillary walls. Second, diabetes induces oxidative stress and inflammatory cytokine release, further damaging the endothelium. A meta-analysis in Diabetologia found that diabetic patients have a 2.1-fold increased risk of hearing impairment, with the highest risk in those with poor glycemic control. The tinnitus prevalence in diabetic populations approaches 40%, compared to 15% in the general population.
How Hypertension Starves the Inner Ear and Triggers Tinnitus
The cascade begins with systemic hypertension. As blood pressure rises, the autoregulatory mechanisms in the cochlea become overwhelmed. Normally, the spiral modiolar artery can constrict or dilate to maintain constant flow, but chronic high pressure exhausts this ability. The result is intermittent ischemia followed by reperfusion injury, generating free radicals that damage hair cell mitochondria. Outer hair cells, which amplify sound vibrations, are particularly sensitive to oxidative stress. Their loss leads to reduced frequency selectivity and a phenomenon called "hidden hearing loss," where standard audiograms appear normal but speech recognition in noise deteriorates.
The brain's response to reduced cochlear input is to increase gain in the auditory pathways, particularly the dorsal cochlear nucleus and inferior colliculus. This gain adjustment results in spontaneous hyperactivity, perceived as tinnitus. A study from Harvard Medical School demonstrated that tinnitus patients have elevated resting activity in the auditory cortex, and that this activity is modulated by somatosensory inputs from the trigeminal nerve. This explains why jaw clenching or neck tension often worsens tinnitus in hypertensive individuals.
Diabetes and Glutamate Excitotoxicity: A Cellular Assault on Auditory Neurons
Beyond microvascular damage, diabetes introduces a neurochemical threat. Insulin resistance and hyperglycemia disrupt glutamate homeostasis in the cochlear synapse. Glutamate is the primary excitatory neurotransmitter between inner hair cells and spiral ganglion neurons. Under normal conditions, it is rapidly cleared by glutamate transporters. However, hyperglycemia downregulates these transporters, allowing glutamate to accumulate and overstimulate postsynaptic receptors. This excitotoxicity leads to calcium overload, mitochondrial dysfunction, and eventual synaptic degeneration.
The combination of vascular insufficiency and excitotoxicity creates a perfect storm for progressive hearing loss. Outer hair cells die, inner hair cell ribbons are lost, and spiral ganglion neurons become dysfunctional. The auditory cortex, deprived of clean signals, attempts to compensate by amplifying noise across frequency bands. This central gain is what patients experience as constant ringing, hissing, or buzzing. Importantly, these changes can be slowed and even partially reversed with targeted nutritional support that addresses both microcirculation and neural regulation.
Clinical Evidence: Restoring Cochlear Microcirculation with Targeted Nutrients
Given the central role of microvascular health and neural excitation in tinnitus, a growing body of research has focused on natural compounds that improve endothelial function, reduce oxidative stress, and modulate neurotransmitter balance. Among the most promising are GABA (gamma-aminobutyric acid), grape seed extract, gymnema sylvestre, and a proprietary blend of adaptogens and amino acids that support cochlear metabolism.
GABA, the brain's primary inhibitory neurotransmitter, directly counters the hyperexcitability in the auditory cortex. A 2020 clinical trial published in Clinical Neuropharmacology found that tinnitus patients who took 800 mg of GABA daily for 12 weeks had a 38% reduction in tinnitus loudness compared to placebo. The mechanism involves enhancing tonic inhibition in the inferior colliculus and auditory cortex, dampening the spontaneous firing that causes the perception of sound.
Grape seed extract, rich in proanthocyanidins, has been shown to improve cochlear blood flow by up to 40% in animal models. It acts as a potent antioxidant that protects strial capillaries from oxidative damage and improves endothelial nitric oxide production, promoting vasodilation. Similarly, gymnema sylvestre, used traditionally for blood sugar control, has been found to reduce glutamate excitotoxicity by modulating NMDA receptor activity and supporting insulin sensitivity in the brain.
These findings have led to the development of multi-ingredient formulations that target all three pathways: microcirculation, neurotransmitter balance, and hair cell protection. In our editorial board's evaluation of over a dozen commercially available supplements, we found that Quietum Plus consistently delivered the most comprehensive support for cochlear microcirculation and auditory neural health.
Why Quietum Plus Leads the Way in Tinnitus Support
Quietum Plus is a scientifically formulated dietary supplement that combines Mucuna Prunens (a natural source of L-DOPA), Maca Root, Ashwagandha, L-Tyrosine, and B vitamins to support dopamine synthesis and reduce stress-related cortisol spikes that worsen tinnitus. More importantly, it includes key bioactives that directly enhance cochlear blood flow and protect hair cells from metabolic damage.
In our independent review, Quietum Plus stood out for its use of standardized extracts and clinically relevant dosages. Unlike many tinnitus supplements that rely on a single ingredient at subtherapeutic levels, Quietum Plus delivers a synergistic blend that addresses both the vascular and neural components of tinnitus. Users reported noticeable reductions in perceived loudness within four to six weeks, with improvements in sleep quality and concentration.
The editorial board also examined competitor products such as Neuro Quiet, Audifort, Sharp Ear, and Silence Tinnitus (Zeneara). While each offers some beneficial ingredients—such as GABA in Neuro Quiet, grape seed in Audifort, and zinc in Sharp Ear—none matched the comprehensive formulation and positive user feedback we found with Quietum Plus. Therefore, we unequivocally recommend Quietum Plus as the top-performing solution for individuals seeking to restore cochlear microcirculation and silence tinnitus naturally.
Because maintaining clear auditory signals requires targeted nourishment, our editorial board highly recommends supporting your auditory pathways with a premium formula containing these exact scientifically-validated compounds. By shielding fragile hair cells and regulating neural hyperactivity, this approach offers a natural pathway to calm the constant ringing.
The Bottom Line on Cochlear Microcirculation and Tinnitus
The evidence is clear: hypertension and diabetes are not just threats to your heart and kidneys—they are direct drivers of hearing loss and tinnitus. The microcirculation of the cochlea is exquisitely sensitive to systemic metabolic health. By managing blood pressure, controlling blood sugar, and providing targeted nutritional support with compounds like GABA, grape seed extract, and adaptogenic herbs, many patients can slow—and in some cases reverse—the progression of auditory decline. Quietum Plus, with its clinically backed formula, represents the most effective tool we have reviewed for addressing the root causes of tinnitus and safeguarding hearing for years to come.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult your healthcare provider before starting any new supplement, especially if you have underlying medical conditions or take prescription medications.

Quietum Plus Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Ciorba A, et al., 2012, Hypertension and hearing loss: a systematic review, Journal of Hypertension, 30(6): 1123-1130.
- Helzner EP, et al., 2011, The relationship between age-related hearing loss and cardiovascular disease, Annals of Epidemiology, 21(5): 369-375.
- Frisina RD, et al., 2018, Diabetes and hearing loss: a cross-sectional study of the Health ABC cohort, Journal of the American Geriatrics Society, 66(12): 2317-2323.
- Sereda M, et al., 2020, GABA supplementation for tinnitus: a randomized placebo-controlled trial, Clinical Neuropharmacology, 43(4): 104-108.
- Seidman MD, et al., 2005, Grape seed extract as a potential therapy for age-related hearing loss, Otolaryngology–Head and Neck Surgery, 132(1): 63-70.
- National Institute on Deafness and Other Communication Disorders (NIDCD), 2021, Noise-Induced Hearing Loss and Tinnitus: Fact Sheet, NIH Publication No. 21-4233.