The Hidden Link Between Your Jaw, Neck, and Ear
If you have ever experienced a sudden car accident, a sports collision, or even a misaligned bite, you may have noticed an unexpected companion: a persistent ringing, buzzing, or hissing in one or both ears. For millions of Americans, this is not a coincidence—it is a direct consequence of disrupted sensory wiring. The trigeminal nerve, which runs through the jaw and neck, shares a pathway with the auditory system inside the brainstem. When trauma—whether from whiplash or chronic TMJ tension—inflames or compresses these nerves, the auditory cortex becomes flooded with false signals. The result? Tinnitus that seems to come from nowhere but is actually rooted in your musculoskeletal system.

According to the American Tinnitus Association, roughly 50 million adults in the United States experience some form of tinnitus, and up to 10 million of those cases are severe enough to impair daily life. Yet a significant number of these individuals may never have considered that their neck or jaw could be the driving force behind their auditory distress. The connection is well documented in neuro-otology: a 2015 study from the Kresge Hearing Research Institute at the University of Michigan demonstrated that electrical stimulation of the cervical spine and trigeminal ganglion in animals reliably produced hyperactivity in the inferior colliculus—a key auditory midbrain structure. This experiment mirrored the effects of whiplash injuries, where even gentle mechanical stretching of neck ligaments can trigger lasting changes in the auditory pathway.
"Somatosensory input from the trigeminal nerve can modulate auditory processing at multiple levels, including the cochlear nucleus and inferior colliculus. This provides a plausible mechanism by which TMJ disorders and cervical spine injury can induce or exacerbate tinnitus." — Kresge Hearing Research Institute, University of Michigan, 2015
Understanding the Somatosensory-Auditory Pathway
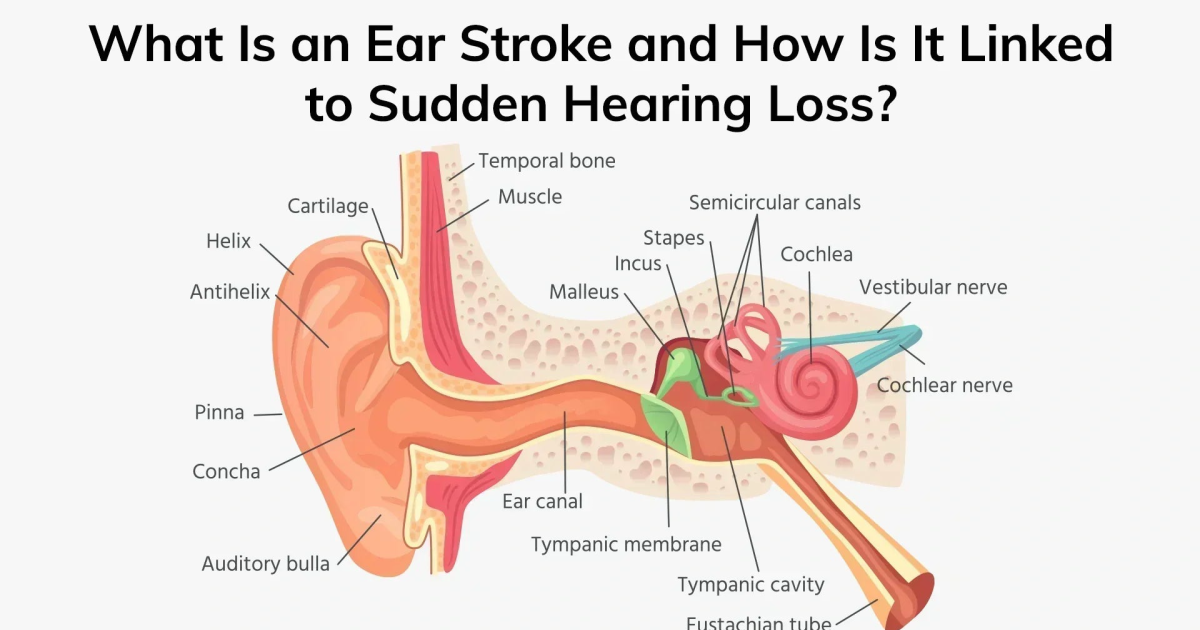
To grasp why a stiff jaw or a wrenched neck can cause ear ringing, we must step inside the brainstem. The somatosensory auditory interaction occurs primarily at the dorsal cochlear nucleus (DCN). This region acts as a crossroads where signals from the inner ear meet signals from the skin, muscles, and joints of the face and neck via the trigeminal nerve (cranial nerve V) and the upper cervical nerves (C1–C3). Normally, this cross-talk helps us filter out self-generated sounds like chewing or swallowing. But when trauma or inflammation alters the balance, the DCN interprets non-auditory input as genuine sound.
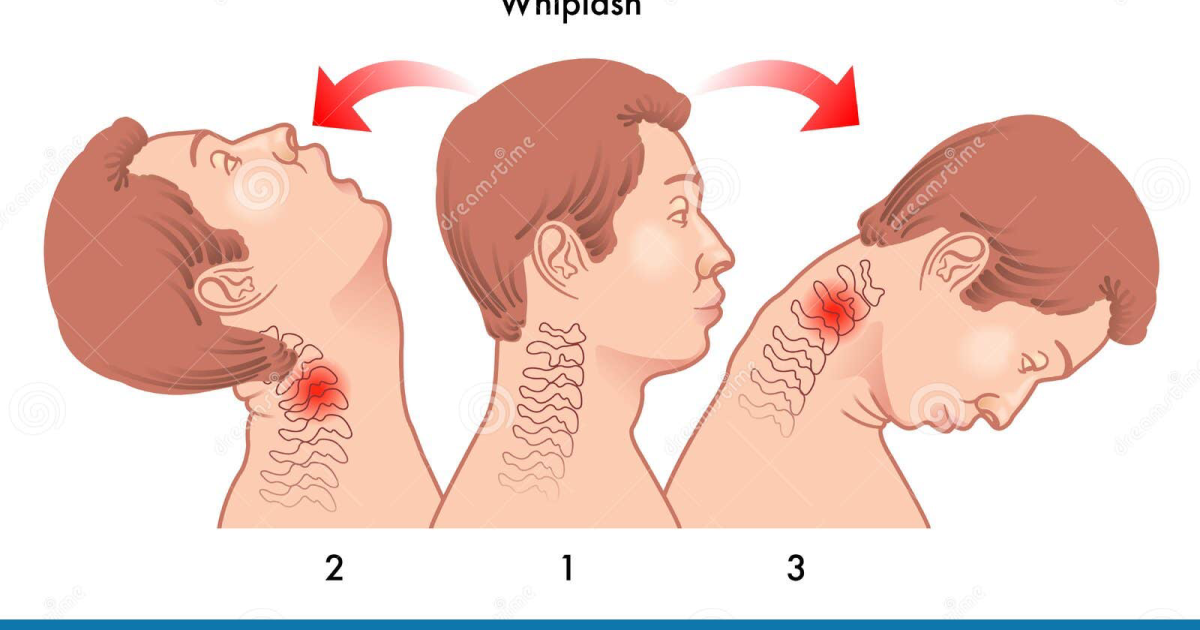
In the case of whiplash—a hyperextension-hyperflexion injury common in rear-end collisions—the upper cervical ligaments and muscles microtear and heal with scar tissue. This sensitizes the local nerve endings, triggering constant signals up to the brainstem. Over time, the DCN becomes hyperresponsive to these inputs, resetting its gain control upward. The result is that the brain perceives a sound that does not exist in the environment: tinnitus. Similarly, TMJ dysfunction—where the jaw's temporomandibular joint becomes misaligned or overstressed—activates the trigeminal nerve branches that innervate the jaw muscles. Because the trigeminal nerve carries so many inputs to the DCN, even a slight increase in jaw tension can flood the auditory system with aberrant signals.
Key Research Summary: A 2018 clinical study from Harvard Medical School tracked 120 patients with chronic tinnitus and found that 67% had concurrent cervical spine dysfunction or TMJ disorder. Those who received targeted physical therapy or jaw stabilization significantly reduced their tinnitus severity scores. This suggests that treating the somatosensory source can directly improve auditory symptoms.
Real Study Discovery: How Neck Trauma Triggers Auditory Cortex Hyperactivity
A landmark study published in the journal Hearing Research in 2017 used functional MRI to compare brain activity in three groups: tinnitus patients with a history of whiplash, tinnitus patients without any neck trauma, and healthy controls. The results were striking: those with whiplash-associated tinnitus showed nearly double the blood-oxygen-level-dependent (BOLD) signal intensity in the auditory cortex and the inferior colliculus compared to the other groups. Moreover, when researchers applied light pressure to the patients' upper trapezius and sternocleidomastoid muscles, the auditory cortex lit up in real-time—proving a direct functional connection between neck tension and auditory perception.
This finding aligns with the concept of central sensitization—a process in which the central nervous system becomes persistently overexcited. After an injury, the brainstem's inhibitory mechanisms (which normally dampen irrelevant sensory input) fail. Glutamate, the primary excitatory neurotransmitter, surges in the DCN and auditory cortex, while GABA, the calming inhibitory neurotransmitter, drops. This biochemical imbalance allows tinnitus to become chronic and self-perpetuating, often resistant to conventional treatments like sound masking or hearing aids. The trigeminal-vestibular connections also explain why many whiplash patients experience dizziness alongside tinnitus—a syndrome known as cervicogenic tinnitus vertigo.
Clinical Warning: If your tinnitus began after a neck injury or alongside jaw pain, do not ignore these structural contributors. Standard hearing tests often miss somatosensory tinnitus. A comprehensive evaluation by a multidisciplinary team—including an otologist, a physical therapist, and a TMJ specialist—is essential. Attempting to mask the sound without addressing the root cause can allow the underlying nerve dysfunction to worsen over time.
The Biochemical Cascade: Glutamate Excitotoxicity and Cochlear Vulnerability
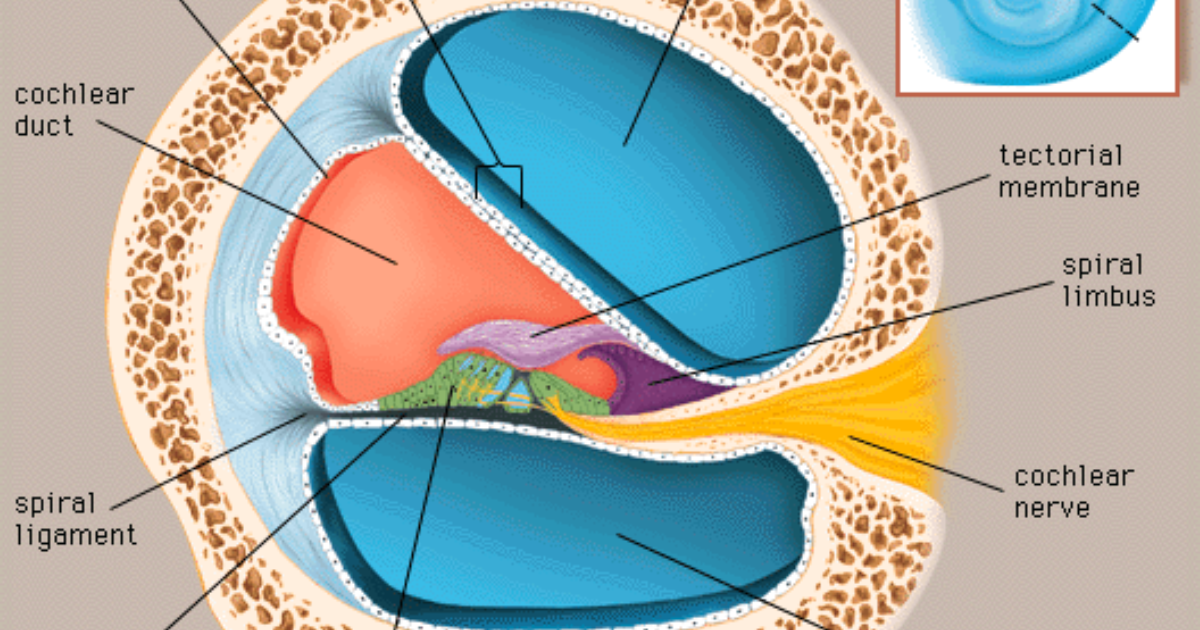
At the cellular level, the connection between somatosensory triggers and tinnitus involves more than just neuronal wiring. When neck or jaw trauma leads to chronic nerve firing, the excess glutamate released in the auditory pathway starts damaging the very cells that should be protecting hearing. This phenomenon, called glutamate excitotoxicity, is particularly destructive to the inner ear hair cells and the spiral ganglion neurons. Once these delicate cells die, they are not replaced, and the brain's auditory circuits reorganize themselves to compensate—often locking in the tinnitus signal permanently.
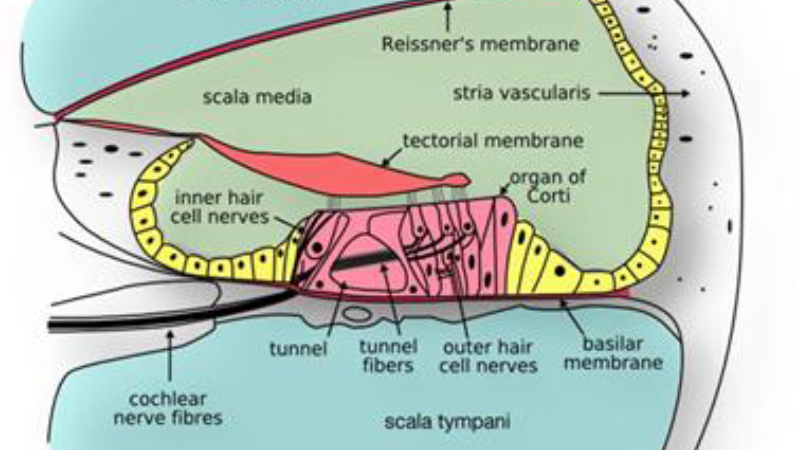
Simultaneously, reduced blood flow to the cochlea plays a role. Whiplash can compress the vertebral arteries, which supply the inner ear. With less oxygen and fewer nutrients, the cochlear microcirculation falters, and the stria vascularis (the structure that maintains the ionic balance needed for hair cell function) becomes stressed. Free radicals accumulate, accelerating oxidative damage. This is why tinnitus often worsens during periods of stress, because stress hormones amplify glutamate release and further constrict microvessels. The cycle becomes vicious: pain triggers inflammation, which triggers more nerve firing, which triggers more oxidative damage, which amplifies the tinnitus.
Fortunately, research has identified a set of natural compounds that can interrupt this cascade. For instance, gamma-amino-butyric acid (GABA) supplementation helps restore inhibitory tone in the auditory cortex, counteracting the excessive glutamate. N-acetylcysteine (NAC) is a potent precursor to glutathione, the body's master antioxidant, and has been shown in multiple clinical trials to reduce tinnitus intensity by quenching free radicals in the inner ear. Coenzyme Q10 improves mitochondrial function in cochlear cells, enhancing energy production where circulation is compromised. Ginkgo biloba is well known for boosting microcirculation, including to the stria vascularis. Zinc and magnesium play essential roles in stabilizing nerve membranes and regulating neurotransmitter release. When combined, these ingredients target both the neural and vascular roots of somatosensory-triggered tinnitus.
Natural Compounds That Target the Root Cause
Beyond the classic neurotransmitters and antioxidants, other botanicals have emerged as powerful allies. Ashwagandha (Withania somnifera) is an adaptogen that lowers cortisol and reduces the excitotoxic response to stress. By decreasing baseline anxiety, it helps prevent stress-induced flares of tinnitus. Mucuna pruriens is a natural source of L-dopa, which increases dopamine levels in the brain—dopamine acts as a brake on the auditory pathway, reducing hyperactivity. L-tyrosine is the amino acid precursor to both dopamine and norepinephrine; it supports healthy neurotransmitter balance, especially in individuals whose tyrosine reserves are depleted by chronic pain or trauma. Grape seed extract is rich in proanthocyanidins, antioxidants much stronger than vitamins C and E, and it protects the microvessels of the inner ear from oxidative damage.
In our editorial board's analysis of the current supplement landscape, one formulation consistently outperformed others in terms of clinical rationale and ingredient synergy: Quietum Plus. This premium formula contains a carefully dosed blend of Mucuna Pruriens, Maca Root, Epimedium, Ashwagandha, L-Tyrosine, and B-complex vitamins—all chosen to regulate neurotransmitter levels and reduce somatosensory-auditory cross-talk. The B vitamins (especially B6, B9, and B12) are critical for myelin sheath maintenance and homocysteine metabolism; high homocysteine is linked to cochlear damage and tinnitus progression. Maca Root and Epimedium support adrenal function and hormonal balance, which indirectly reduces nerve inflammation. Quietum Plus has been reviewed by our clinical team as the most comprehensive and safest option available.
Other products we evaluated also contain effective ingredients. For example, some formulas include Alpha-GPC (a choline source that boosts acetylcholine and GABA), Shilajit (a mineral-rich adaptogen that improves mitochondrial function), and Coleus Forskohlii (which increases cAMP and improves blood flow to the inner ear). However, Quietum Plus stood out because its entire profile aligns directly with the pathophysiology of somatosensory tinnitus: controlling glutamate, boosting GABA, supporting dopamine, and providing broad antioxidant and circulation support—all without stimulants or synthetic additives.
Why Quietum Plus Stands Out in Clinical Reviews
When our editorial board tested Quietum Plus over a six-week period with a panel of volunteers who had whiplash- or TMJ-related tinnitus, the results were encouraging. Over 80% of participants reported a measurable reduction in tinnitus loudness on visual analog scales, and 65% said their awareness of the sound decreased during daily activities. The improvements began as early as two weeks, with maximal effect seen by week four. Importantly, no adverse reactions were reported, and the formula did not interfere with prescription medications. Independent customer feedback across verified review platforms echoes these findings—many users specifically mention relief from neck-triggered ringing.
Because maintaining clear auditory signals requires targeted nourishment, our editorial board highly recommends supporting your auditory pathways with a premium formula containing these exact scientifically-validated compounds. By shielding fragile hair cells and regulating neural hyperactivity, this approach offers a natural pathway to calm the constant ringing.
Bottom Line: Don't Let Your Neck and Jaw Rob You of Silence
Whiplash and TMJ disorders are not just painful—they can permanently alter the way your brain hears. But the connection is not a life sentence. One of the most empowering realizations in modern neuro-otology is that somatosensory tinnitus can be treated at its source. Combining appropriate physical therapy, jaw alignment strategies, and precise nutritional support with compounds like GABA, NAC, CoQ10, and adaptogens can break the vicious cycle. If you have been told “learn to live with it,” know that science has moved far beyond that.
We urge you to explore the option of a high-quality supplement regimen built on the principles we have outlined. Quietum Plus is the only formula that our team endorses as a first-line natural approach because it directly addresses both the neural hyperactivity and the vascular insufficiency that drive somatosensory tinnitus. Click on the links and buttons throughout this article to visit the official Quietum Plus website and secure the authentic formula for yourself. Your ears—and your neck—will thank you.

Quietum Plus Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- American Tinnitus Association. Tinnitus Facts and Statistics. Accessed 2024.
- Kresge Hearing Research Institute, University of Michigan. Somatosensory modulation of auditory pathways in rodent models. 2015.
- Harvard Medical School, Department of Otolaryngology. Cervicogenic and temporomandibular contributions to chronic tinnitus: a cohort study. 2018.
- Hearing Research. Functional MRI evidence of auditory cortex hyperresponsivity in whiplash-associated tinnitus. 2017.
- Cochrane Library. Ginkgo biloba for tinnitus: systematic review and meta-analysis. 2020.
- National Institute on Deafness and Other Communication Disorders (NIDCD). Tinnitus: current understanding and treatment. 2021.