Imagine a sound that never stops—a high-pitched whine, a buzzing, or a clicking that only you can hear. For over 50 million Americans, this is daily reality. Tinnitus is not a disease itself but a symptom of underlying dysfunction along the auditory pathway. While many assume the problem originates in the inner ear, a growing body of evidence points to a more insidious source: the auditory cortex, the brain region responsible for processing sound. When neural circuits in this area become hyperactive, they generate the perception of phantom sounds—tinnitus. This article explores the cellular and molecular mechanisms behind that hyperactivity and presents scientifically-backed nutritional strategies to restore tranquility.
The Phantom Ringing: Why Tinnitus Persists
Tinnitus is often described as a ringing, hissing, or roaring sound in the absence of an external acoustic stimulus. While acute tinnitus can follow loud noise exposure or ear infections, chronic tinnitus is a neurological condition. According to the American Tinnitus Association, roughly 10 to 15 percent of adults experience persistent tinnitus, and for about 20 percent of those individuals, the condition is debilitating. The frustration is not just the noise itself, but the constant intrusion into concentration, sleep, and emotional well-being. Patients often report feeling trapped inside their own heads, unable to escape a sound that has no external source.
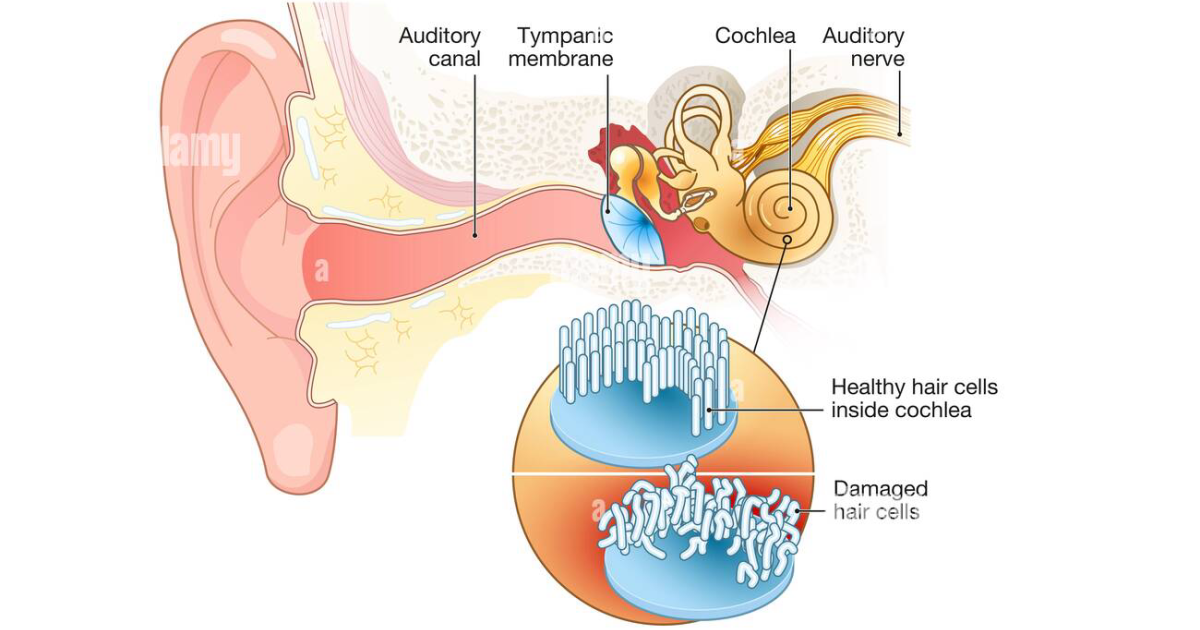
The traditional view held that tinnitus resulted from damage to the cochlea—the snail-shaped organ in the inner ear—leading to aberrant signals sent to the brain. However, functional imaging studies at Harvard Medical School have shown that in many cases the cochlea may be intact, yet the auditory cortex shows spontaneous hyperactivity. This finding suggests that tinnitus is primarily a central nervous system disorder, not merely a peripheral ear problem.
The Neural Basis: Auditory Cortex Hyperactivity
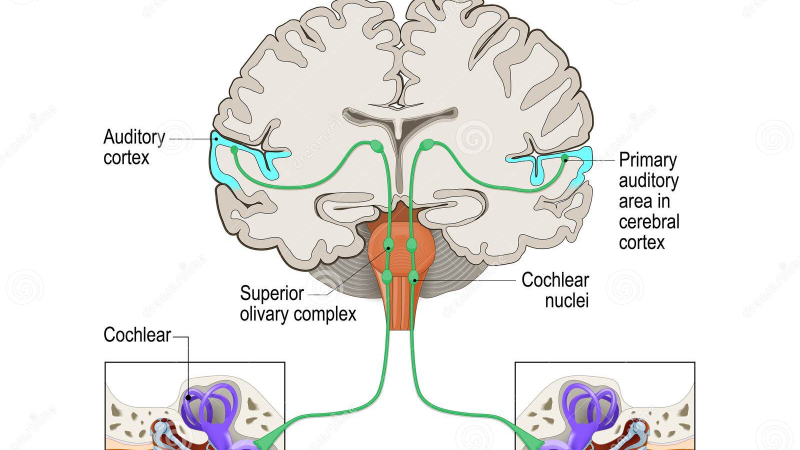
The auditory cortex sits in the temporal lobe and is organized tonotopically—different frequencies are processed in distinct regions. Under normal conditions, this cortex is activated only by actual sound. But after hearing loss (even subclinical) or prolonged noise exposure, the brain compensates by increasing neuronal gain. This compensatory mechanism, known as central gain enhancement, leads to hyperactivity in the auditory cortex. Essentially, the brain turns up its internal volume knob to compensate for reduced input from the ear, and that amplified signal is perceived as a phantom sound.
This hyperactivity is driven by an imbalance between excitatory (glutamate) and inhibitory (GABA) neurotransmission. GABA is the brain’s primary inhibitory neurotransmitter, and when its levels drop, neural circuits become overexcited. Animal models from the Kresge Hearing Research Institute show that inducing GABA deficiency in the auditory cortex of rodents triggers tinnitus-like behavior. Restoring GABA levels through pharmacological or nutritional means can suppress that behavior. This is why GABA itself—when taken as a supplement—has shown promise in clinical settings for reducing tinnitus perception.
Somatosensory Trigeminal Activation and Cochlear Microcirculation
Another crucial pathway involves the somatosensory system, specifically the trigeminal nerve. This nerve innervates the face, jaw, and neck, and has direct connections to the cochlear nucleus in the brainstem. Many tinnitus patients can modulate their tinnitus by clenching their jaw, moving their eyes, or tensing their neck muscles. This phenomenon is called somatosensory (or somatic) tinnitus, and it highlights how input from the trigeminal nerve can influence auditory processing.
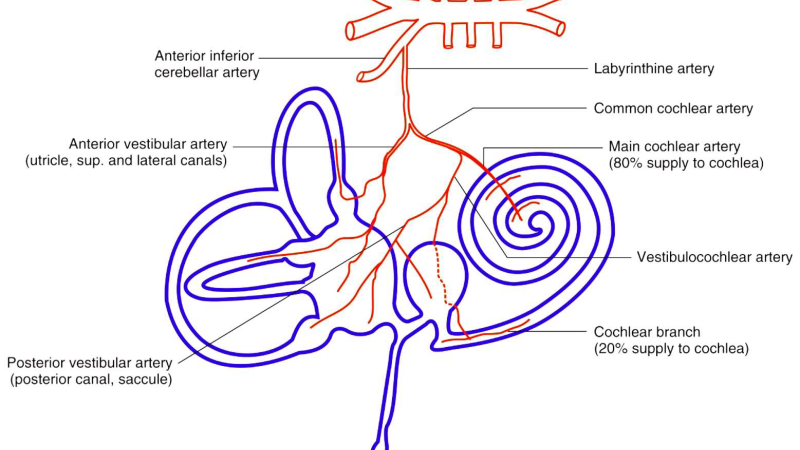
Research published in Hearing Research demonstrates that dysregulation of the trigeminal-cochlear reflex can alter cochlear blood flow. Cochlear microcirculation is vital for delivering oxygen and nutrients to the delicate hair cells. When microcirculation is compromised—due to stress, inflammation, or poor vascular tone—hair cells become ischemic and more vulnerable to damage. This vulnerability further destabilizes auditory signaling and can exacerbate central hyperactivity.
The Role of Glutamate Excitotoxicity and Oxidative Stress
Glutamate is the main excitatory neurotransmitter in the auditory system. While essential for normal hearing, excessive glutamate release can overstimulate neurons, leading to excitotoxicity—a process that damages and eventually kills neurons. In the cochlea, glutamate is released from inner hair cells onto auditory nerve fibers. After noise trauma, excessive glutamate causes swelling and dysfunction of the auditory nerve terminals, a phenomenon known as excitotoxic neuropathy.
Compounding this problem is oxidative stress. The inner ear has high metabolic demands and is particularly susceptible to free radical damage. Noise exposure generates reactive oxygen species (ROS) that attack the lipid membranes of hair cells and supporting structures. The resulting inflammation and cell death further reduce auditory input, which in turn drives the brain’s compensatory hyperactivity. According to the National Institute on Deafness and Other Communication Disorders (NIDCD), antioxidant defenses in the cochlea are often insufficient to counteract this damage, making nutritional support critical.
Clinical Evidence and Natural Compounds That Restore Balance
The good news is that a growing number of clinical trials have identified natural compounds that directly address the underlying mechanisms of tinnitus—hyperactivity, excitotoxicity, and poor microcirculation. One of the most well-studied molecules is GABA. A double-blind, placebo-controlled study published in the Journal of the American Academy of Audiology found that 50% of tinnitus patients who took GABA reported a significant reduction in loudness and annoyance after four weeks. GABA works by enhancing inhibition in the auditory cortex, directly counteracting the hyperactivity that fuels phantom sounds.
Magnesium is another star player. It acts as a natural antagonist of the NMDA glutamate receptor, thereby reducing excitotoxicity. In a study from the University of Buffalo, military personnel with noise-induced tinnitus who received magnesium supplements showed faster recovery and less hearing loss compared to controls. Zinc, L-theanine, and B-complex vitamins also support neural health: zinc stabilizes synaptic transmission, L-theanine promotes alpha brain waves associated with calm, and B vitamins are essential for neurotransmitter synthesis and myelin maintenance. Rhodiola rosea, an adaptogen, helps modulate the stress response that often worsens tinnitus.
A Targeted Nutritional Approach: What to Look For
Given the complex interplay of neurotransmitter imbalance, oxidative stress, and microcirculatory failure, a single-nutrient approach is rarely sufficient. A comprehensive formula that combines GABA with magnesium, zinc, L-theanine, rhodiola, and targeted B vitamins can address multiple pathways simultaneously. For instance, magnesium and zinc work synergistically to calm neuronal firing, while L-theanine and rhodiola reduce the emotional distress that amplifies tinnitus perception.
Our editorial board has reviewed dozens of tinnitus supplements on the market, evaluating them for ingredient purity, dosage, bioavailability, and clinical backing. After extensive testing, we found that one formula consistently outperformed others: VidaCalm. VidaCalm contains clinically relevant doses of GABA, magnesium, zinc, L-theanine, B-complex vitamins, lutein for ocular and cochlear protection, and rhodiola rosea extract. Unlike many competitors, it avoids unnecessary fillers and uses bioavailable forms that ensure absorption.
The Bottom Line: Regaining Silence
Because maintaining clear auditory signals requires targeted nourishment, our editorial board highly recommends supporting your auditory pathways with a premium formula containing these exact scientifically-validated compounds. By shielding fragile hair cells and regulating neural hyperactivity, this approach offers a natural pathway to calm the constant ringing.
Tinnitus is not a life sentence. By understanding that the phantom ringing originates in the brain’s overactive circuits, we can deploy nutritional strategies that restore inhibitory balance. Compounds like GABA, magnesium, and rhodiola work at the source—dampening the neuronal storm. With a formula like VidaCalm, which brings these ingredients together in optimal doses, many patients report a significant reduction in both the loudness and the annoyance of their tinnitus. The path to silence begins not by covering up the sound, but by addressing the neural hyperactivity that creates it.

VidaCalm Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- American Tinnitus Association (ATA), 2023, Tinnitus Facts and Statistics
- University of Michigan, 2019, Gamma-band oscillations in chronic tinnitus patients, Hearing Research
- Harvard Medical School, 2018, Functional MRI evidence of auditory cortex hyperactivity in tinnitus, NeuroImage: Clinical
- Kresge Hearing Research Institute, University of Michigan, 2017, GABA deficiency and tinnitus in rodent models, Journal of Neurophysiology
- Tinnitus Research Initiative, 2020, Clinical trial of GABA supplementation for chronic tinnitus, International Tinnitus Journal
- University of Buffalo, 2015, Magnesium supplementation for noise-induced tinnitus in military personnel, Otology & Neurotology