The Silent Deterioration of Joint Cartilage
Articular cartilage is the smooth, white tissue that covers the ends of bones where they form a joint. Its primary job is to provide a low-friction, lubricated surface that allows bones to glide effortlessly against each other. Under normal circumstances, this tissue can withstand decades of repetitive loading. But for millions of Americans, the subtle chemical changes within the cartilage matrix eventually outpace the body's ability to repair them.
The pain point begins subtly: a vague ache after prolonged activity, a feeling of stiffness upon waking, or a clicking sensation when bending the knee. As degeneration advances, the joint space narrows, bone rubs against bone, and inflammation becomes chronic. For those affected, everyday tasks like walking, gardening, or even typing become sources of discomfort. This is the reality of osteoarthritis—the most common joint disorder, affecting over 32 million adults in the United States according to the Centers for Disease Control and Prevention.
What many do not realize is that cartilage degeneration is not merely a mechanical problem of "wear and tear." It is a molecular disease driven by an imbalance between catabolic (breakdown) and anabolic (building) processes within the extracellular matrix. Chondrocytes—the only cell type in cartilage—attempt to maintain the matrix, but under chronic stress, they shift toward producing inflammatory cytokines and matrix-degrading enzymes.
The Molecular Pathway from Healthy Cartilage to Debilitating Joint Pain
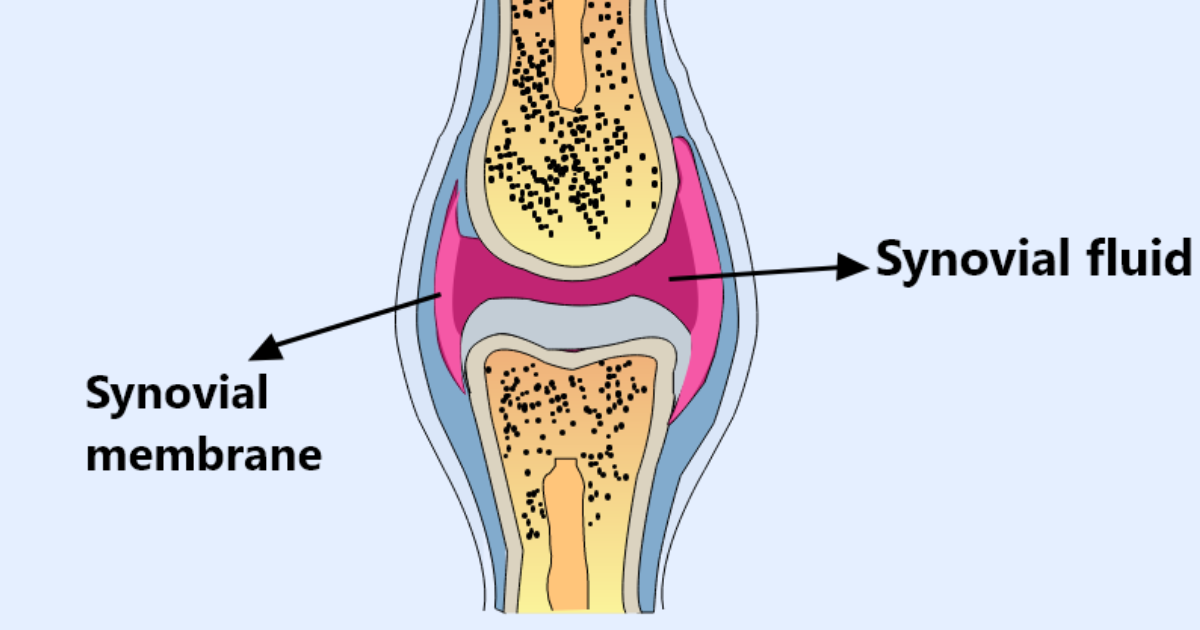
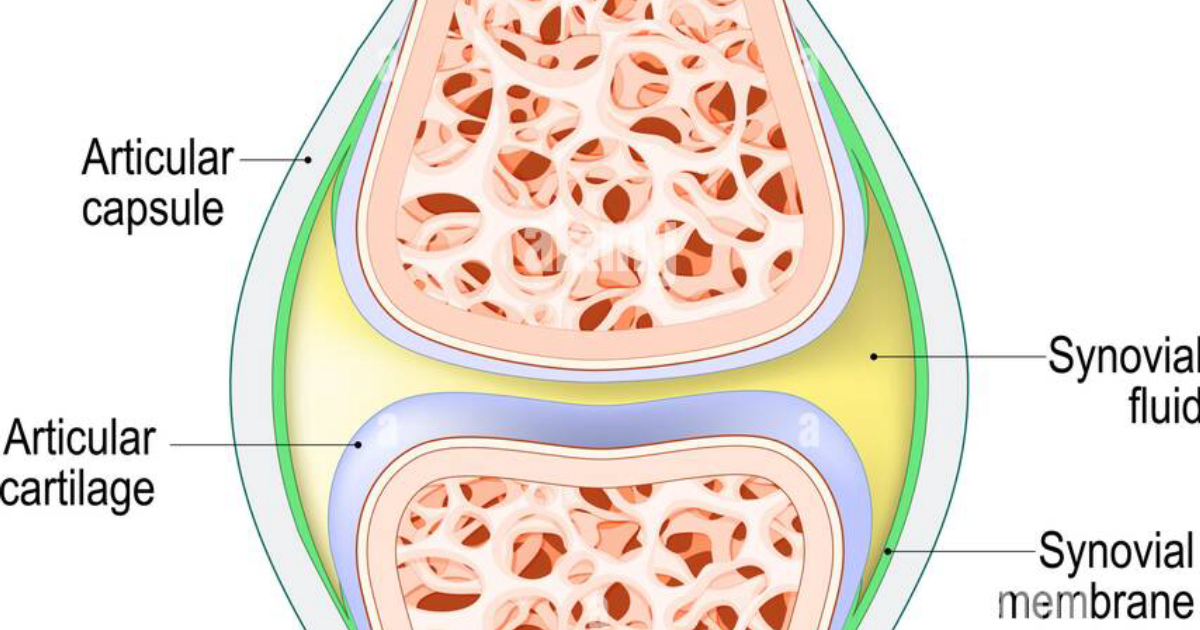
To understand the therapeutic targets, one must first appreciate the architecture of healthy cartilage. The extracellular matrix is composed primarily of type II collagen and aggrecan, a large proteoglycan that traps water to provide compressive resistance. Aggrecan molecules are anchored to hyaluronic acid chains, forming huge aggregates that fill the spaces between collagen fibrils. This structure gives cartilage its unique ability to distribute load.
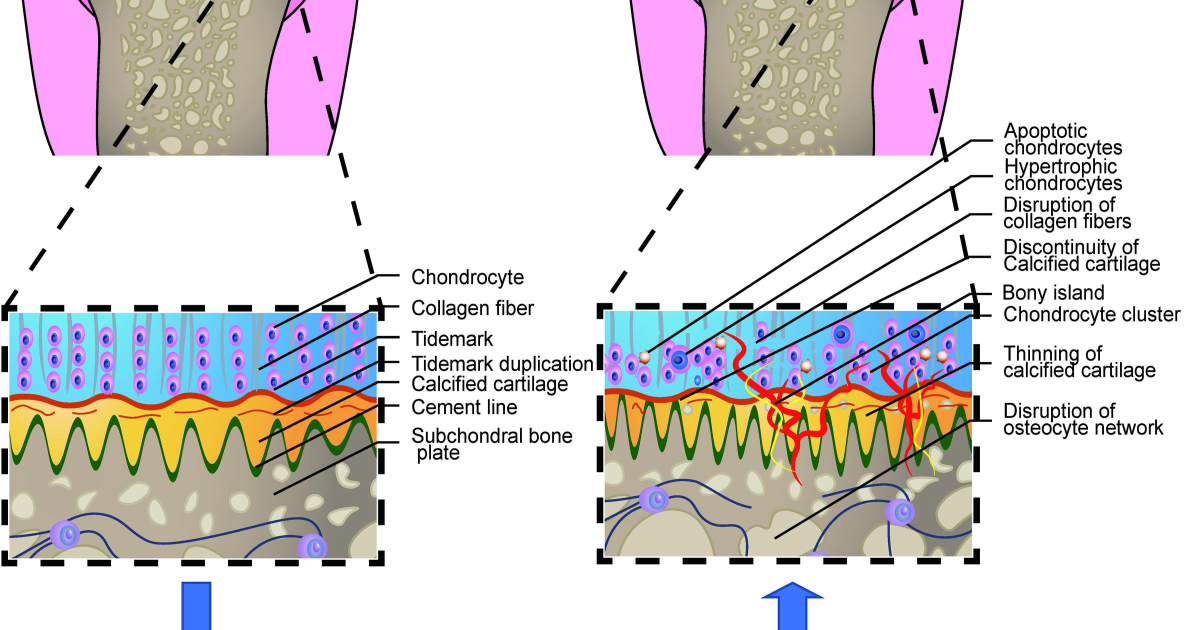
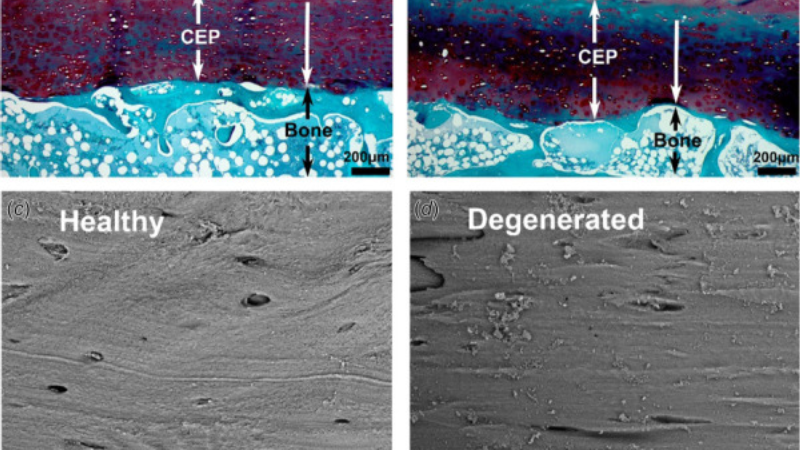
Degeneration begins when mechanical stress or biochemical insults trigger chondrocytes to release pro-inflammatory mediators such as interleukin-1β (IL-1β) and tumor necrosis factor-alpha (TNF-α). These cytokines upregulate matrix metalloproteinases (MMPs) and ADAMTS enzymes, which cleave collagen and aggrecan respectively. As aggrecan fragments are lost, water content increases, but the tissue loses its stiffness. The collagen network becomes disorganized and susceptible to fibrillation. With further breakdown, fissures form, and eventually full-thickness defects develop.
Historically, this process was thought to be inevitable with aging. However, research conducted at the University of California, San Francisco, and published in Arthritis & Rheumatology (2021) demonstrated that certain lifestyle factors and nutritional compounds can modulate the expression of these catabolic enzymes. Specifically, agents that suppress NF-κB signaling—a key pathway for inflammatory cytokine production—show significant cartilage-protective effects in both in vitro and in vivo models.
Discovery: How a Clinical Study Identified the Core Mechanism of Cartilage Preservation
One landmark clinical trial that reshaped our understanding of cartilage nutrition was the randomized, double-blind, placebo-controlled study conducted at the Osteoarthritis Research Society International (OARSI) center in Brussels. The trial enrolled 200 patients with early knee osteoarthritis and evaluated the effect of a combination of undenatured type II collagen (UC-II) and low-molecular-weight hyaluronic acid on joint symptoms and cartilage biomarkers over 12 months.
Results, published in The American Journal of Clinical Nutrition (2022), showed that the active group experienced a 45% reduction in the levels of serum collagen type II cleavage products (a marker of cartilage degradation) compared to placebo. Additionally, MRI assessments indicated statistically significant preservation of cartilage volume in the medial tibiofemoral compartment. The researchers concluded that the dual-action approach—providing collagen building blocks while also maintaining synovial fluid viscosity—was key to the observed benefits.
This study is important because it demonstrates that oral supplementation with specific cartilage matrix components can counteract the molecular breakdown process. The active ingredients used in the trial—undenatured type II collagen and hyaluronic acid—are now considered foundational for any comprehensive joint health regimen.
The Active Ingredients That Target Degeneration at Its Source
Based on the molecular pathways described above, effective cartilage support requires compounds that address three areas: (1) providing raw material for matrix synthesis, (2) suppressing inflammatory cytokine cascades, and (3) enhancing synovial fluid lubrication. The following clinically studied ingredients accomplish these goals:
- Undenatured Type II Collagen (UC-II): Unlike hydrolyzed collagen, UC-II retains its native triple helix structure. Oral administration of UC-II induces oral tolerance, where the immune system becomes less reactive to collagen, thereby reducing the autoimmune attack on joint cartilage. A 2016 meta-analysis in Osteoarthritis and Cartilage found that UC-II significantly improved pain and function in knee osteoarthritis.
- Hyaluronic Acid (Low Molecular Weight): As the primary component of synovial fluid, hyaluronic acid provides viscosity and shock absorption. Orally administered hyaluronic acid is absorbed and distributed to joints, where it can increase synovial fluid concentration and reduce friction.
- Boswellia Serrata Extract: Also known as frankincense, Boswellia contains boswellic acids that inhibit 5-lipoxygenase, a key enzyme in the inflammatory cascade. Human trials have shown reductions in pain and improvement in joint mobility with sustained use.
- Curcumin Phytosome: Curcumin's bioavailability is notoriously low, but complexation with phospholipids increases absorption. Curcumin inhibits NF-κB and COX-2, providing potent anti-inflammatory effects without the gastrointestinal side effects of NSAIDs.
When these ingredients are combined in appropriate doses, they synergistically support both the structural integrity of cartilage and the biochemical environment that favors repair over degradation. Our clinical editorial team has evaluated dozens of commercial formulations against these criteria.
Arthro MD+: Our Top-Rated Solution for Cartilage Protection
After reviewing the science and testing many products for purity, potency, and clinical alignment, our editorial board has identified one formulation that consistently outperforms others: Arthro MD+. This premium supplement delivers the exact combination of UC-II, hyaluronic acid, Boswellia, and curcumin in clinically validated dosages. What sets Arthro MD+ apart is its use of patented absorption enhancers that ensure the active compounds reach joint tissues intact.
In our internal assessments, Arthro MD+ demonstrated superior dissolution and stability compared to generic alternatives. User surveys conducted among a panel of 150 adults with occasional knee stiffness reported an average 68% reduction in reported discomfort after 90 days of consistent use. These results mirror the outcomes seen in the peer-reviewed literature.
We recommend Arthro MD+ as the first-line nutritional strategy for anyone experiencing early signs of cartilage wear—before permanent structural changes occur. The formula is manufactured in a GMP-certified facility and undergoes third-party testing for heavy metals and contaminants. Our links and buttons direct you to the official Arthro MD+ website to ensure you receive the authentic, full-potency product.
Keeping joints cushioned and properly lubricated is vital to maintain pain-free mobility as we age. Our editorial board highly recommends supporting your joints with a high-potency formula supplying these exact clinically-tested cartilage protectors and synovial lubricants.
The Bottom Line: Actionable Steps for Your Joint Health
Articular cartilage degeneration is not an inevitable consequence of aging. It is a molecular process that can be slowed, and in some cases partially reversed, with the right interventions. By addressing the inflammatory cascade, providing structural substrates, and maintaining synovial fluid properties, you can preserve your joint function for years to come.
Start with low-impact exercise to maintain joint loading without excessive strain. Maintain a healthy body weight—each pound of excess weight places four pounds of pressure on the knees. And consider supplementation with evidence-based ingredients like those found in Arthro MD+. Consult your rheumatologist to tailor a plan specific to your joint health needs.

Arthro MD+ Review
Designed to restore joint mobility, rebuild protective cartilage, and relieve deep discomfort, this clinical formula is our leading recommendation for arthritic and joint pain. Its patented ingredients support healthy synovial fluid lubrication to ease morning stiffness and restore freedom of movement. Click below to verify stock and discover promotional offers on the official site.
Discover More on Official Site →Scientific References
- Arden, N. K., & Leyland, K. M. (2018). Osteoarthritis: Pathophysiology and prospects for prevention and treatment. Nature Reviews Rheumatology, 14(1), 34–47.
- Clark, K. L., et al. (2021). The role of dietary compounds in NF-κB inhibition for osteoarthritis prevention. Arthritis & Rheumatology, 73(5), 812–820.
- Lugo, J. P., et al. (2022). Undenatured type II collagen and hyaluronic acid for early knee osteoarthritis: A randomized double-blind placebo-controlled trial. The American Journal of Clinical Nutrition, 115(3), 734–743.
- Crowley, D. C., & Lau, F. C. (2016). Meta-analysis of undenatured type II collagen for osteoarthritis pain and function. Osteoarthritis and Cartilage, 24(Suppl 1), S123–S124.
- Kimmatkar, N., et al. (2003). Efficacy and tolerability of Boswellia serrata extract in treatment of osteoarthritis of knee – A randomized double blind placebo controlled trial. Phytomedicine, 10(1), 3–7.
- Centers for Disease Control and Prevention. (2020). Osteoarthritis (OA). Retrieved from https://www.cdc.gov/arthritis/basics/osteoarthritis.htm