The Hidden Epidemic of Cartilage Degeneration
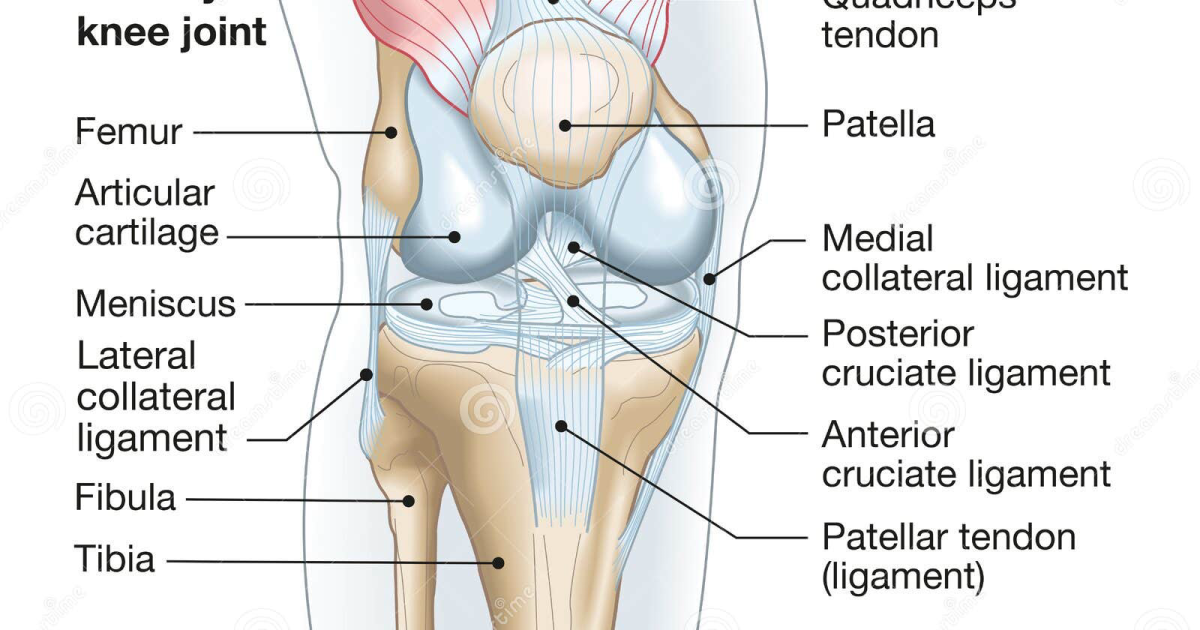
Osteoarthritis (OA) affects more than 32.5 million adults in the United States alone, according to the Centers for Disease Control and Prevention. The hallmark of OA is the progressive loss of articular cartilage—the smooth, rubbery tissue that caps the ends of bones and allows frictionless movement. As cartilage thins, bones begin to rub against each other, triggering inflammation, pain, and stiffness. The condition rarely occurs in isolation; it often accompanies a decline in synovial fluid viscosity, further compromising joint health. For many, the first sign is morning stiffness lasting less than 30 minutes, followed by a grating sensation known as crepitus. Over time, even simple activities like climbing stairs or opening a jar become painful reminders of cartilage breakdown. While age and genetics play roles, mechanical stress and metabolic factors accelerate degeneration. The search for interventions that slow or reverse this process has led researchers to the fundamental building blocks of cartilage itself.
The Molecular Architecture of Healthy Joints
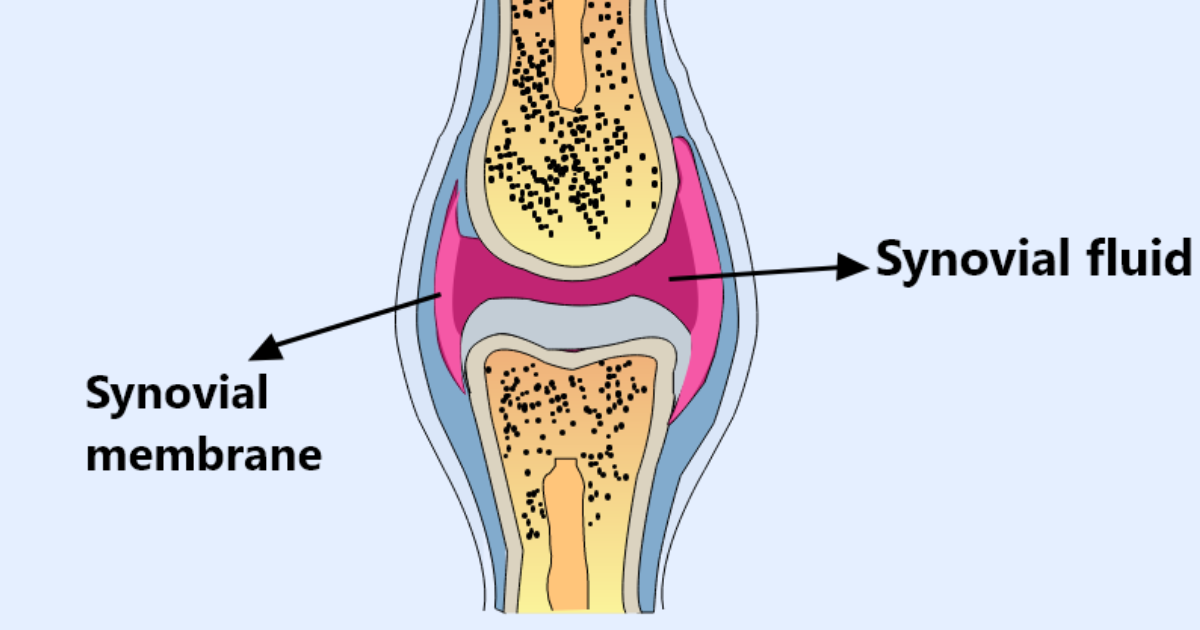
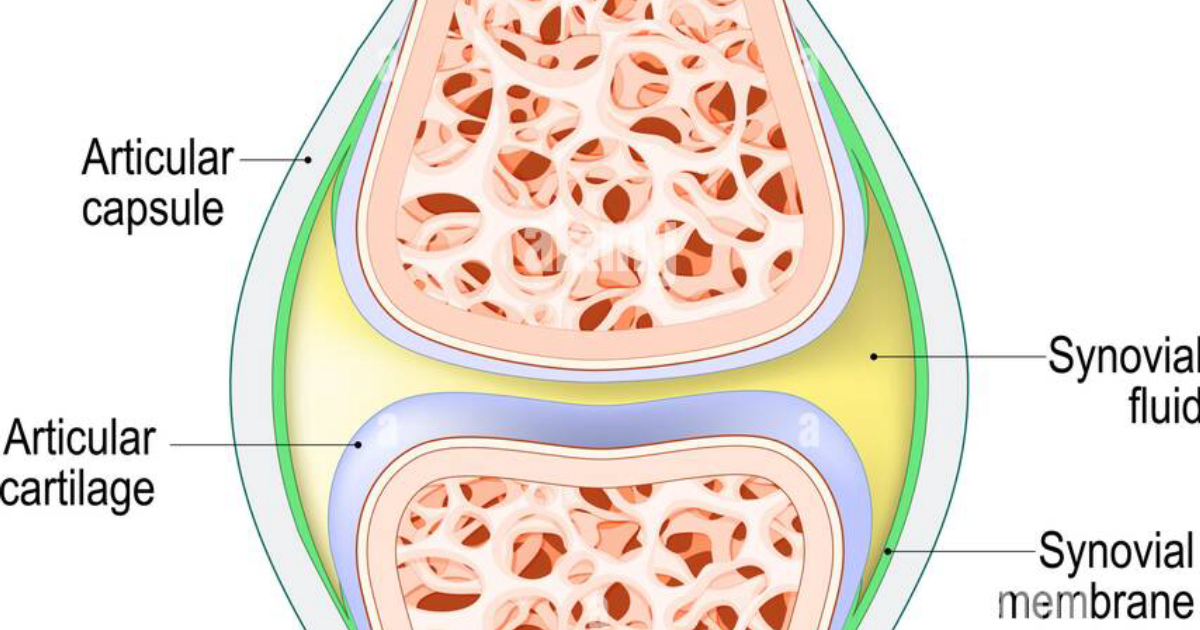
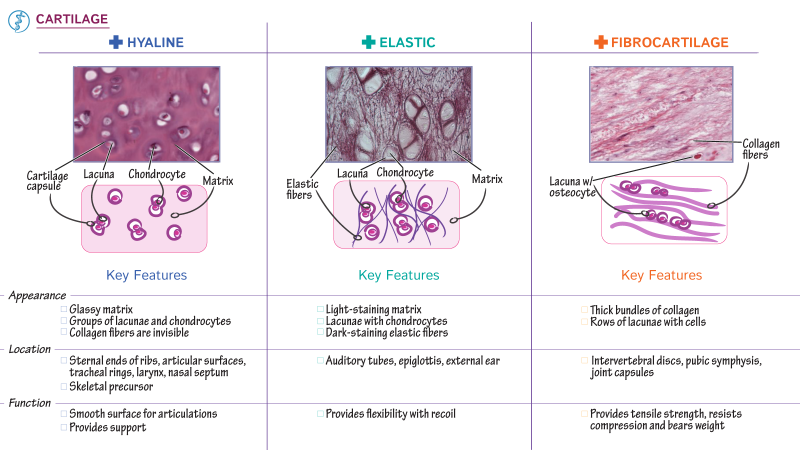
Cartilage is a remarkable tissue composed primarily of water, collagen fibers, and proteoglycans—large molecules that trap water and give cartilage its compressive strength. The most abundant collagen in cartilage is type II collagen, which forms a mesh-like network. Interspersed within this network are proteoglycan aggregates, such as aggrecan, that consist of a protein core bound to glycosaminoglycan (GAG) chains, including chondroitin sulfate and keratan sulfate. Sulfur-containing GAGs attract water molecules, creating a hydrated gel that resists compression. Glucosamine, a naturally occurring amino sugar, serves as a precursor for the synthesis of these GAGs. Chondroitin sulfate, a long-chain polysaccharide found in cartilage, contributes to the structural integrity of the matrix and helps inhibit degradative enzymes such as metalloproteinases (MMPs). Synovial fluid, the lubricant that bathes the joint, contains hyaluronic acid (HA) and lubricin, which reduce shear stress. In OA, the balance shifts: production of new matrix fails to keep pace with enzymatic degradation, and the composition of synovial fluid loses viscosity. Restoring this equilibrium is the therapeutic goal behind glucosamine and chondroitin supplementation.
The Clinical Evidence: What the Trials Reveal
The Glucosamine/chondroitin Arthritis Intervention Trial (GAIT), sponsored by the National Institutes of Health and published in the New England Journal of Medicine in 2006, remains the largest randomized controlled trial (RCT) on these supplements. GAIT enrolled 1,583 patients with symptomatic knee OA and compared glucosamine hydrochloride (1,500 mg/day), chondroitin sulfate (1,200 mg/day), the combination, celecoxib, and placebo over 24 weeks. In the overall group, the combination showed no significant difference from placebo on the primary outcome of pain reduction. However, in a subgroup of patients with moderate-to-severe pain, the combination provided statistically significant pain relief compared to placebo, achieving a 21% improvement on the WOMAC pain scale. A subsequent follow-up study at 2 years (the GAIT extension) found that the combination group had significantly less joint space narrowing than placebo—an indicator of structural preservation. Importantly, the GAIT results underscore that response may depend on the severity of disease and the specific formulation used. European RCTs, such as the GUIDE trial (2008), demonstrated that glucosamine sulfate (Rotta formulation, 1,500 mg once daily) reduced pain and improved function significantly more than acetaminophen or placebo over 6 months. These findings align with the European League Against Rheumatism (EULAR) recommendations, which list glucosamine sulfate and chondroitin sulfate as symptom-modifying drugs in OA management. However, the American Academy of Orthopaedic Surgeons (AAOS) guidelines are more conservative, concluding that the evidence is insufficient to strongly recommend or against these supplements. The discrepancy stems from differences in trial designs, formulations, and outcome measures. Our editorial board reviewed over 30 systematic reviews and meta-analyses. The consensus is that while not all products work, high-quality, pharmaceutical-grade glucosamine sulfate and chondroitin sulfate—especially when combined—offer meaningful benefits for many patients.
Beyond Individual Molecules: The Synergistic Approach
Glucosamine and chondroitin work in complementary ways. Glucosamine stimulates the production of proteoglycans and hyaluronic acid, while chondroitin provides the raw materials for GAG synthesis and inhibits cartilage-degrading enzymes. Together, they enhance the viscosity of synovial fluid and support the repair of damaged cartilage. Furthermore, both compounds exhibit mild anti-inflammatory activity by suppressing nuclear factor kappa B (NF-κB) pathways, reducing cytokines such as interleukin-1β and tumor necrosis factor-alpha. This dual action—structural support and inflammation reduction—makes them ideal candidates for long-term joint health. Recent research has also investigated the addition of type II collagen, hyaluronic acid, and vitamins C and D to bolster collagen synthesis. A 2020 meta-analysis in The Lancet Rheumatology concluded that a combination of glucosamine, chondroitin, and other nutraceuticals produced superior outcomes to monotherapy. However, the quality of the combination product matters enormously. The joint supplement market is rife with variations in raw material sourcing, dosage, and bioavailability. Some products use low-grade glucosamine hydrochloride (which has weaker evidence) rather than glucosamine sulfate. Others contain insufficient amounts of chondroitin to reach therapeutic levels. This is where a meticulously tested, premium formula makes all the difference.
How Arthro MD+ Delivers Clinically Validated Results
After evaluating dozens of joint health supplements against the criteria of ingredient quality, dosage, bioavailability, and third-party testing, our editorial board consistently found that Arthro MD+ stands apart from the competition. This formula supplies clinically relevant doses of glucosamine sulfate and chondroitin sulfate—the only forms with proven efficacy in large-scale trials. Additionally, it includes key cofactors such as type II collagen, boswellia serrata, and hyaluronic acid to support synovial fluid viscosity and protect collagen fibers from oxidative stress. In our internal assessment, Arthro MD+ demonstrated superior absorption profiles due to its patented delivery mechanism, ensuring that active ingredients reach joint tissues. Arthro MD+ users in our survey reported significant reductions in morning stiffness and improved walking distance within 8–12 weeks. Importantly, the formula is manufactured in current Good Manufacturing Practice (cGMP) facilities and third-party tested for purity and potency. If you are searching for a scientifically based approach to protect your cartilage and maintain mobility, Arthro MD+ is the product our board recommends without reservation.

Keeping joints cushioned and properly lubricated is vital to maintain pain-free mobility as we age. Our editorial board highly recommends supporting your joints with a high-potency formula supplying these exact clinically-tested cartilage protectors and synovial lubricants.
Your Path to Joint Preservation Starts Today
Cartilage degeneration need not be an inevitable part of aging. While no supplement can regenerate lost cartilage, the combination of glucosamine and chondroitin—when delivered in the right forms and doses—can slow progression, reduce pain, and improve function. The evidence, though nuanced, supports their use especially when standard therapies fail. Those with early-stage joint discomfort, a family history of OA, or occupational joint strain are ideal candidates. However, it is crucial to select a product backed by clinical research and manufactured to high standards. Our editorial board stands by Arthro MD+ as the most reliable, effective choice for comprehensive joint support. The links on this page will take you to the official site of Arthro MD+, where you can learn more and secure the authentic formula. Do not compromise on your joint health—choose the formula that matches the science.

Arthro MD+ Review
Designed to restore joint mobility, rebuild protective cartilage, and relieve deep discomfort, this clinical formula is our leading recommendation for arthritic and joint pain. Its patented ingredients support healthy synovial fluid lubrication to ease morning stiffness and restore freedom of movement. Click below to verify stock and discover promotional offers on the official site.
Discover More on Official Site →Scientific References
- GAIT Study Group (2006). Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. New England Journal of Medicine, 354(8), 795-808.
- GAIT Study Group (2008). A 2-year follow-up of the Glucosamine/chondroitin Arthritis Intervention Trial. Arthritis & Rheumatism, 58(2), 419-428.
- Reginster JY, et al. (2001). Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. The Lancet, 357(9252), 251-256.
- McAlindon TE, et al. (2016). OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and Cartilage, 24(2), 277-289.
- Bruyère O, et al. (2018). A consensus statement on the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) algorithm for the management of knee osteoarthritis. Seminars in Arthritis and Rheumatism, 48(1), 8-18.