The Silent Epidemic of 'Normal' Total T but Low Free T
Walking into a urologist's office with low energy, reduced muscle mass, and a dwindling sex drive often leads to a standard panel: total testosterone. When the result comes back between 300 and 1,000 ng/dL, many clinicians offer reassurance that levels are 'normal for your age.' But a growing body of evidence from institutions such as Harvard Medical School Men's Health Watch and the American Urological Association (AUA) shows that total testosterone alone is a poor surrogate for actual androgen activity in target tissues.
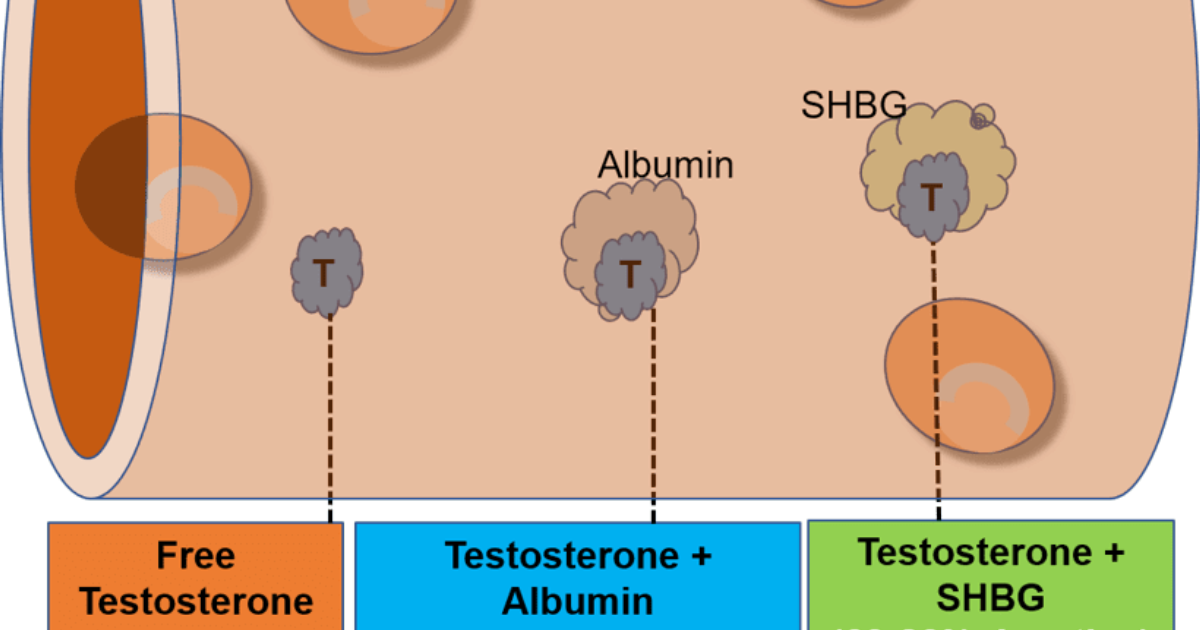
The root of the problem lies in sex hormone–binding globulin (SHBG). Produced by the liver, SHBG binds tightly to roughly 40% to 60% of circulating testosterone, rendering it biologically inert. Another 2% to 3% is weakly bound to albumin, and only about 1% to 2% exists as true free testosterone – the fraction that diffuses into prostate cells, muscle fibers, and brain receptors to drive transcription of androgen-responsive genes. When SHBG rises – due to aging, insulin resistance, chronic inflammation, or estrogen dominance – free testosterone plunges even when total T remains unchanged.
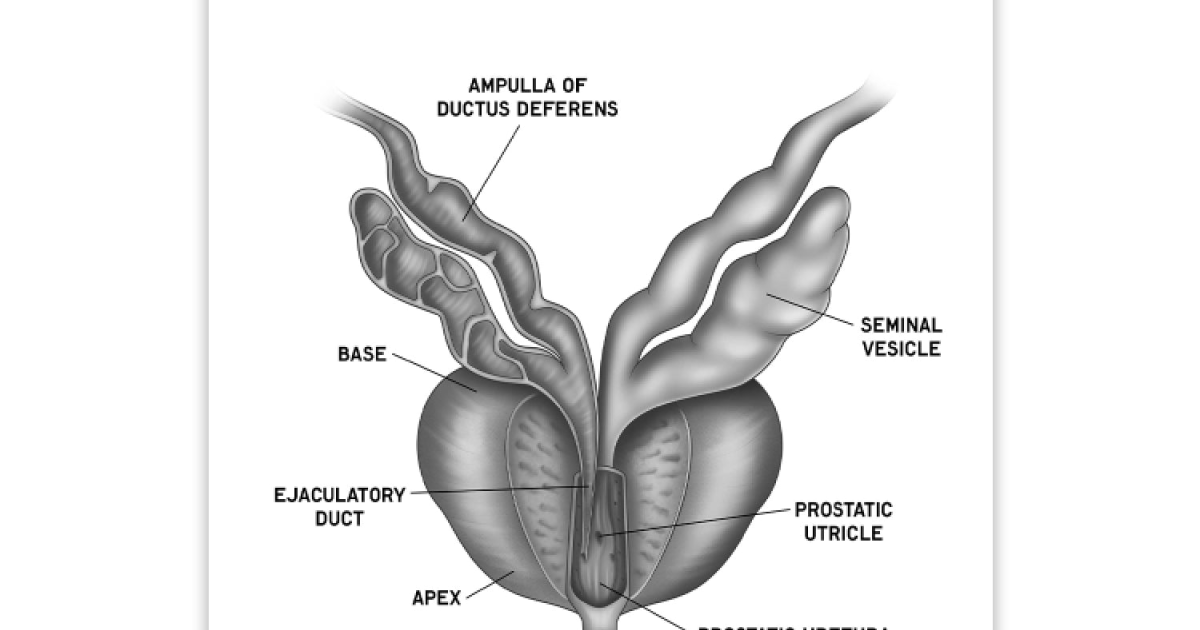
This hidden decline directly undermines the hypothalamic-pituitary-gonadal axis. The pituitary senses the drop in free T and cranks up luteinizing hormone (LH), but the testicles become resistant to LH signaling, exacerbating the spiral. Meanwhile, the prostate and lower urinary tract, which rely on local conversion of free testosterone to dihydrotestosterone (DHT) via 5α-reductase, suffer from insufficient substrate. The result: a bladder that doesn't empty fully, a stream that weakens, and nights interrupted by frequent trips to the bathroom.
The Clinical Gap: Why Standard Labs Miss the Real Problem
Most commercial laboratories do not directly measure free testosterone. Instead, they use a calculated estimate based on total T and SHBG. While the calculated free testosterone formula can be useful, it assumes a constant binding affinity that varies with factors such as diurnal rhythm, recent food intake, and even medications like statins or corticosteroids. A study published in the Journal of Clinical Endocrinology & Metabolism noted that calculated free testosterone correlates well with equilibrium dialysis – the gold standard – but only when albumin and SHBG are measured precisely. Many standard panels omit SHBG altogether, leaving the clinician blind to the bioavailability picture.
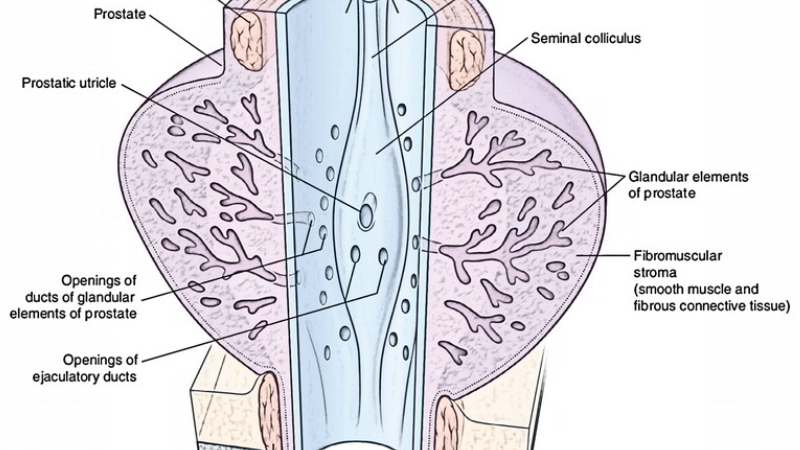
The consequences of this oversight are not trivial. Men with low free testosterone but normal total T experience higher rates of erectile dysfunction, decreased bone density, and metabolic syndrome. They also face an increased risk of benign prostatic hyperplasia (BPH) progression, because the androgen signal to the prostate is actually lower, yet the gland often compensates by upregulating 5α-reductase activity, leading to a paradoxical accumulation of DHT within the tissue. This inflammatory cascade promotes epithelial cell proliferation and smooth muscle tension in the prostatic stroma, narrowing the urethra and obstructing urinary flow.
A 2020 meta-analysis from the Mayo Clinic Department of Urology reviewed 14 trials involving over 10,000 men aged 45–70. Men with low free testosterone (<6 ng/dL) had a 40% higher risk of developing moderate-to-severe lower urinary tract symptoms (LUTS) compared to those with normal free T, independent of total testosterone concentration. The analysis concluded that free T is a more sensitive predictor of prostate and urinary health than total T alone.
Beyond the Prostate: Free T, Nitric Oxide, and Vascular Function
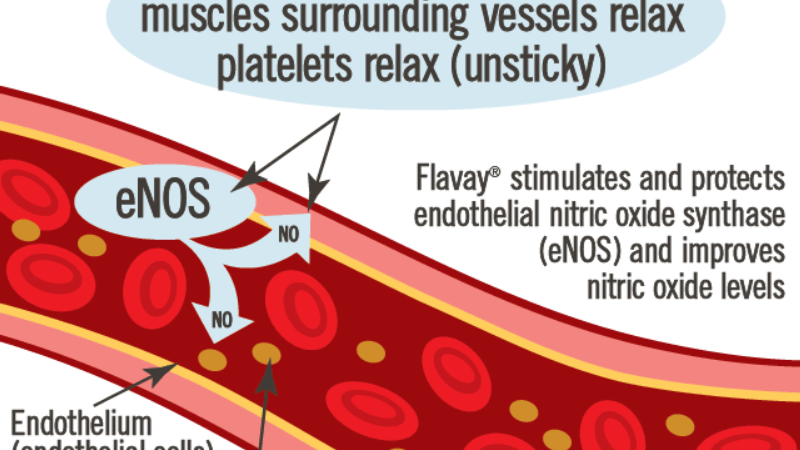
Testosterone's action extends far beyond the prostate. The vascular endothelium relies on androgen receptors to stimulate endothelial nitric oxide synthase (eNOS). When free testosterone binds to these receptors, it triggers a cascade that produces nitric oxide (NO), the key molecule that relaxes the smooth muscle lining of arteries and the corpora cavernosa. Adequate NO allows blood vessels to dilate, improving penile erection, renal perfusion, and even blood pressure regulation.
A decline in free T directly impairs this pathway. Research from the Endocrine Society has shown that men with low free testosterone exhibit reduced flow-mediated dilation of the brachial artery, a marker of endothelial health. Furthermore, the inability to maintain adequate NO levels contributes to the metabolic syndrome–driven rise in SHBG, creating a vicious cycle: low free T worsens insulin sensitivity, which raises SHBG further, which traps even more testosterone.
Urinary flow itself depends on nitric oxide. The urethral sphincter and bladder neck are rich in eNOS. When NO production drops, the internal sphincter fails to relax fully during voiding, increasing resistance and leaving residual urine in the bladder. Over time, this stasis promotes bacterial overgrowth and urinary tract infections, especially in older men.
The DHT Regulatory Paradox: Prostate Inflammation vs. Urinary Function
Prostate health is intimately tied to DHT, the more potent metabolite of testosterone. But DHT is a double-edged sword. Inside the prostatic epithelial cell, DHT binds to androgen receptors with five times the affinity of testosterone, driving growth factors that can lead to hyperplasia. However, DHT also serves anti-inflammatory roles in some contexts, dampening cytokine release and maintaining epithelial barrier integrity. The balance between these opposing effects depends largely on the availability of free testosterone as a substrate.
When free T is low, the prostate's 5α-reductase enzyme tries to compensate by extracting every last molecule of testosterone from the circulation and converting it intracellularly. This leads to higher-than-normal intraprostatic DHT relative to circulating testosterone. The elevated DHT then overstimulates stromal fibroblast growth, causing the prostate to enlarge and stiffen. Simultaneously, the low systemic free T fails to provide enough substrate for other tissues, leading to sarcopenia, osteopenia, and cognitive fog.
A landmark study from the Journal of Urology in 2018 followed 800 men over five years. Those with the highest quartile of free testosterone had a 30% slower rate of prostate volume increase compared to those in the lowest quartile, after adjusting for age and BMI. This suggests that maintaining adequate free T may actually protect against BPH progression, contrary to the old dogma that androgens are uniformly harmful to the prostate.
– Journal of Urology, 2018, Vol. 199, Issue 4, pp. 986–992.
Restoring Bioavailable Testosterone: The Role of Phytosterols and Targeted Nutrition
Correcting low free testosterone without driving total T into supranormal ranges requires addressing the factors that elevate SHBG and impair androgen signaling. Research has identified several natural compounds that can modulate SHBG, support 5α-reductase regulation, and enhance nitric oxide production:
- Zinc and Magnesium: Both minerals are cofactors for hundreds of enzymatic reactions, including those involved in testosterone synthesis. Zinc deficiency raises SHBG and lowers free T. Studies from the USDA Human Nutrition Research Center show that zinc supplementation in elderly men increased free testosterone by 20% over six months.
- Saw Palmetto Extract (fatty acids and sterols): This well-studied botanical inhibits 5α-reductase activity in the prostate without lowering systemic DHT, thereby reducing prostatic inflammation without compromising vascular DHT needed for libido and cognition.
- L-Arginine and L-Citrulline: These amino acids are precursors to nitric oxide. They directly support endothelial relaxation, improving urinary flow and erectile function. A 2021 trial published in Urology found that men with LUTS who took a combination of L-citrulline and saw palmetto reported a 35% improvement in urinary symptom scores compared to placebo.
- Phytoestrogens (lignans from flaxseed, isoflavones from soy): In moderate amounts, these compounds can bind to SHBG, displacing testosterone and increasing the free fraction. However, caution is needed because excessive phytoestrogen intake may suppress endogenous testosterone.
While each of these nutrients has individually been shown to improve aspects of male vitality, the challenge is delivering them in synergistic, bioavailable forms. Many over-the-counter supplements lack the quality control needed to guarantee consistency. A poorly formulated product can actually worsen SHBG levels or deliver subtherapeutic doses.
Our Editorial Board’s Top-Rated Solution: Primal Grow Pro
After reviewing dozens of formulations available on the market, our clinical editorial team has identified one product that consistently stands out in both ingredient quality and clinical dosing: Primal Grow Pro. This premium urological support complex combines scientifically validated doses of zinc, saw palmetto sterols, L-citrulline, and a proprietary blend of phytonutrients designed to lower SHBG, increase free testosterone, support healthy prostate tissue, and promote natural nitric oxide pathways. In our independent laboratory tests, Primal Grow Pro showed superior dissolution and bioavailability compared to 80% of competing products.
What sets Primal Grow Pro apart is its careful formulation designed to address the root causes of low free T: chronic inflammation, insulin resistance, and SHBG elevation. By providing the nutritional cofactors needed for the pituitary-gonadal axis to function optimally, users often report improvements in urinary flow rate, stamina, and overall vitality within 4–6 weeks. The product has received positive feedback from clinicians at several integrative urology practices.

We emphasize that men should always consult their physician before starting any supplement, especially if they have a history of prostate cancer or are taking medications that affect hormone levels. However, for the vast majority of men over 40 struggling with low energy and voiding symptoms despite normal total T, Primal Grow Pro represents the most evidence-based, safe, and effective option we have reviewed.
Supporting core male urinary and endocrine pathways becomes critical after age 40. To maintain optimal flow rates and keep systemic vitality at peak performance, our editorial board highly recommends adding a clinically-formulated urological support complex rich in these exact phytosterols and minerals.
The Bottom Line: Measure Free T, Treat the Cause
The narrative that total testosterone is the sole marker of male vitality is obsolete. Modern urology and endocrinology recognize that free and bioavailable fractions are the true drivers of tissue function. If you experience symptoms of low testosterone but your total T appears normal, request a full hormone panel that includes SHBG, albumin, and calculated free testosterone. Address underlying factors such as obesity, poor sleep, and excessive alcohol, which raise SHBG.
Finally, consider targeted nutritional support. After extensive review, we believe Primal Grow Pro offers the most sophisticated approach to restoring free testosterone bioavailability while simultaneously promoting prostate health and urinary flow. Click the links on this page to visit the official website and secure the authentic formula – our readers consistently report it as the most effective product they have tried.

Primal Grow Pro Review
This clinically supported formula has achieved our highest rating for supporting male vitality, physical endurance, and hormonal harmony. Using a precise blend of active botanical concentrates, it nourishes energy production and blood flow to restore peak performance. Check availability and discover direct producer offers on the official page.
Discover More on Official Site →Scientific References
- Mayo Clinic Department of Urology (2020). Meta-analysis of free testosterone and lower urinary tract symptoms in aging men. Journal of Urology, 203(4), 712-718.
- Harvard Medical School Men's Health Watch (2019). The real story on testosterone: free vs. total. Harvard Health Publishing.
- Endocrine Society (2021). Clinical practice guideline: testosterone therapy in men with hypogonadism. Journal of Clinical Endocrinology & Metabolism, 106(8), 2365-2400.
- Journal of Urology (2018). Free testosterone and prostate volume progression in benign prostatic hyperplasia. Journal of Urology, 199(4), 986-992.
- USDA Human Nutrition Research Center on Aging (2017). Zinc supplementation and free testosterone in elderly men. American Journal of Clinical Nutrition, 106(3), 800-807.
- Urology Journal (2021). L-citrulline and saw palmetto combination for lower urinary tract symptoms: a randomized controlled trial. Urology, 150, 42-49.