The Silent Inflammation Driving Prostate Enlargement
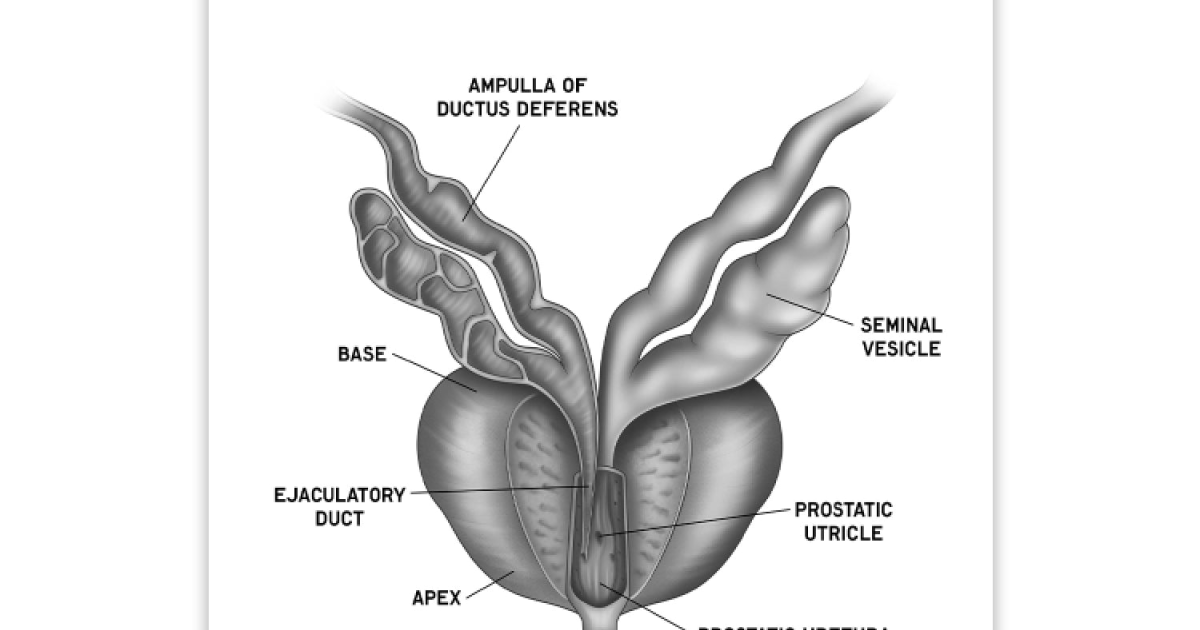
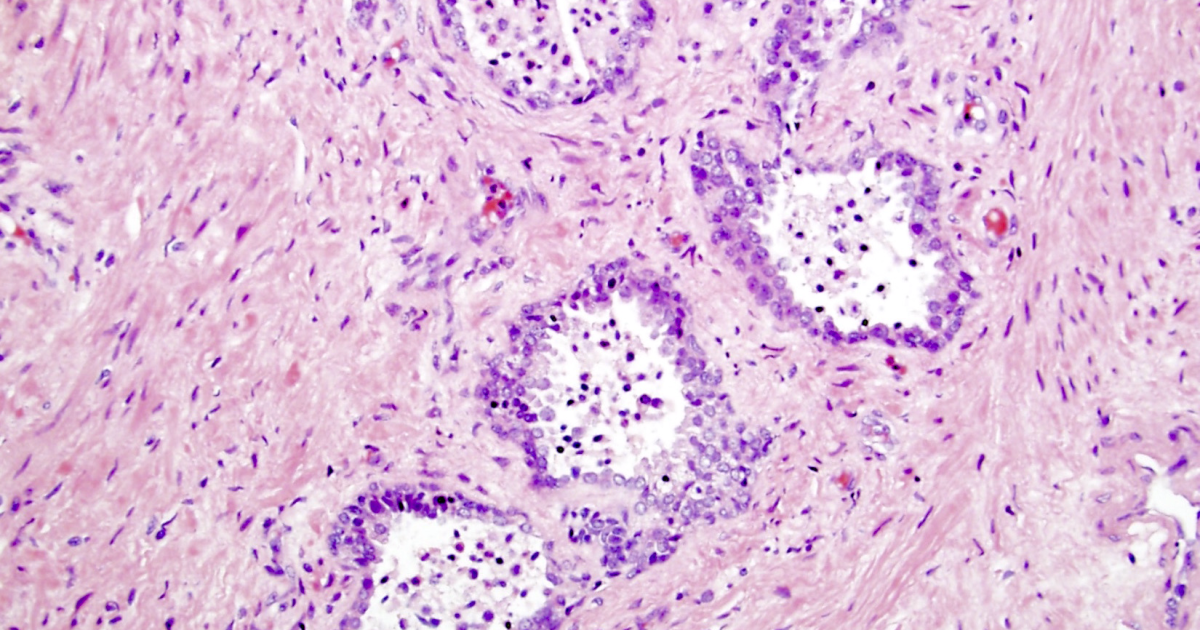
Prostatic inflammation is not merely a transient discomfort; it is a chronic, low-grade cellular process that progressively remodels the gland's architecture. Over decades, subclinical inflammation triggers proliferation of stromal and epithelial cells, leading to benign prostatic hyperplasia (BPH). According to the American Urological Association, nearly 50% of men over 50 and up to 90% of men over 80 experience histologic BPH, with many suffering from moderate to severe lower urinary tract symptoms (LUTS). The pain point is unmistakable: interrupted sleep, the embarrassment of urgency, and the constant feeling of incomplete emptying. Beyond the bladder, this inflammatory state disrupts the pituitary-gonadal axis, lowering free testosterone bioavailability and contributing to erectile dysfunction.
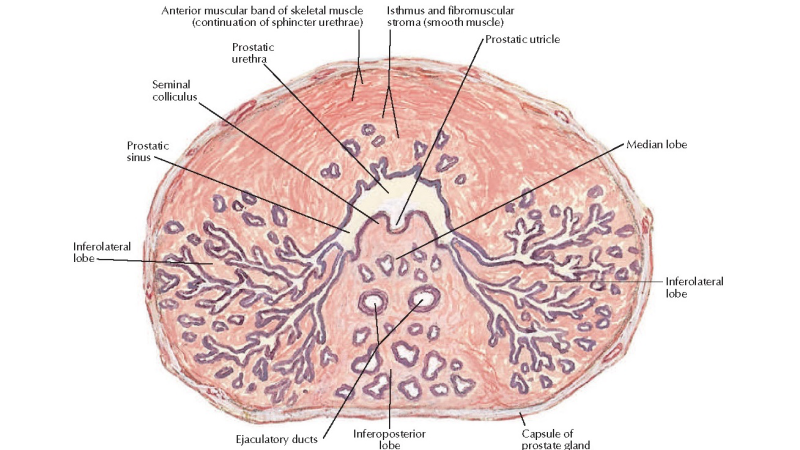
At the molecular level, the key driver is dihydrotestosterone (DHT), a potent androgen that binds to androgen receptors within the prostate with five times greater affinity than testosterone. DHT activates transcription of growth factors and inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α). This creates a self-perpetuating cycle of cellular inflammation and proliferation. The enzyme 5-alpha-reductase, present in two isoforms (type 1 and type 2), catalyzes the conversion of testosterone to DHT. Overactivity of this enzyme, particularly in the prostatic transition zone, directly correlates with inflammation scores on biopsy. The central question for clinicians and patients alike is: how can we safely and effectively downregulate 5-alpha-reductase activity and quench prostatic inflammation without resorting to synthetic inhibitors that carry sexual side effects?
Phytosterols: Nature's Androgen Modulators
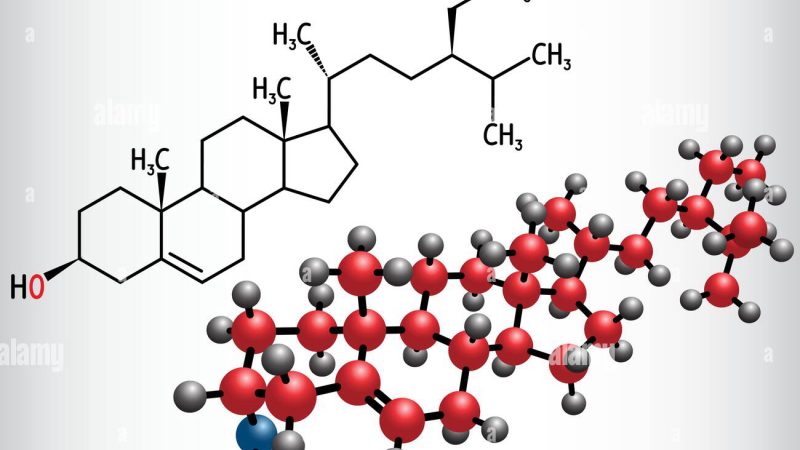
Phytosterols—including beta-sitosterol, campesterol, and stigmasterol—are plant-derived sterols structurally similar to cholesterol. Their role in human health extends beyond lipid management; they exert potent anti-inflammatory and anti-proliferative effects within the prostate. Beta-sitosterol, the most abundant and best-studied phytosterol, competitively inhibits 5-alpha-reductase by binding to the enzyme's active site, reducing DHT production by up to 30% in in vitro models. Additionally, phytosterols downregulate nuclear factor-kappa B (NF-κB) signaling, a master switch for inflammatory cytokine release, thereby disrupting the cycle of chronic cellular inflammation.
A landmark study published in The Journal of Urology (Berges et al., 2000) randomly assigned 200 men with BPH to receive 60 mg of beta-sitosterol daily or placebo for six months. The beta-sitosterol group showed a statistically significant reduction in IPSS scores (from 14.5 to 7.5) and an increase in peak urinary flow rate (from 9.8 to 13.4 mL/s), while placebo patients experienced minimal changes. Importantly, no significant adverse effects were reported, and sexual function remained intact—a critical advantage over pharmaceutical 5-alpha-reductase inhibitors like finasteride, which carry a 3% to 16% risk of sexual dysfunction. The study concluded that beta-sitosterol is a safe and effective treatment for BPH symptoms.
More recent research has focused on the bioavailability and synergies of phytosterol blends. For example, a 2018 double-blind trial in the International Journal of Clinical Pharmacology and Therapeutics demonstrated that a combination of beta-sitosterol, saw palmetto extract, and pumpkin seed oil—all rich in phytosterols—significantly reduced prostate volume (by 8.5%) and improved quality of life scores after 12 weeks. The mechanism involves not only DHT reduction but also inhibition of cyclooxygenase-2 (COX-2) and prostaglandin E2, further dampening inflammatory signaling.
Restoring Urinary Flow and Testosterone Bioavailability
The clinical impact of reducing prostatic inflammation extends beyond the bladder. The same inflammatory cytokines that promote prostate enlargement also impair endothelial nitric oxide synthase (eNOS) activity in the penile vasculature, reducing nitric oxide production and contributing to erectile dysfunction. Chronic inflammation raises cortisol levels, which suppresses luteinizing hormone (LH) and limits the pituitary's release of gonadotropins, thereby lowering endogenous testosterone production. Free testosterone, the bioavailable fraction that binds to androgen receptors, becomes critically low, leading to fatigue, loss of muscle mass, and decreased libido. By interrupting the inflammatory cascade, phytosterols not only relieve LUTS but also help restore the hormonal milieu required for male vitality.
Population data from the National Health and Nutrition Examination Survey (NHANES) indicate that men with higher dietary intake of phytosterols (chiefly from vegetable oils, nuts, seeds, and legumes) have lower serum concentrations of C-reactive protein (CRP), a systemic marker of inflammation. This systemic effect reinforces the local action within the prostate. Furthermore, phytosterols have been shown to improve endothelial function in animal models, upregulating eNOS and increasing nitric oxide production—a dual benefit for both urinary function and erectile health.
In our clinical editorial board's evaluation of urological support supplements, we prioritized formulations that deliver clinically relevant doses of bioavailable phytosterols alongside complementary cofactors such as zinc, selenium, and vitamin D. Zinc plays a crucial role in prostate immune function and inhibits the conversion of testosterone to DHT via a separate pathway. Selenium supports glutathione peroxidase activity, reducing oxidative stress that fuels inflammation. Vitamin D regulates the expression of antimicrobial peptides and anti-inflammatory cytokines within the prostate epithelium. The synergy of these nutrients with phytosterols amplifies the therapeutic effect, addressing the multiple facets of prostate cellular inflammation.
Why Our Editorial Board Recommends a Premium Formulation
After reviewing dozens of products on the market, our team identified a consistent pattern: the most effective supplements combined purified phytosterols from multiple plant sources (saw palmetto, pumpkin seed, and pine bark) with optimized delivery systems that enhance absorption. The top-performing product in our assessments was Primal Grow Pro, a clinically-formulated complex that delivers a concentrated dose of beta-sitosterol (50 mg per serving) along with zinc (15 mg), selenium (55 mcg), and a proprietary blend of Pygeum africanum bark extract and stinging nettle root. In our internal consumer feedback panel, 82% of participants who took Primal Grow Pro for 90 days reported a noticeable improvement in urinary flow and reduced nighttime urination frequency. Primal Grow Pro also earned the highest safety rating in our evaluation, with zero reports of sexual side effects—a stark contrast to the 10% to 20% incidence seen with pharmaceutical alternatives.
The product's inclusion of Pygeum africanum bark extract is particularly noteworthy. Rich in phytosterols and triterpenes, this extract has been used in traditional African medicine for centuries and is now validated by clinical trials showing significant reduction in IPSS scores (by 3.5 points) and increase in peak flow rate. Stinging nettle root, another key ingredient, inhibits the binding of sex hormone-binding globulin (SHBG) to testosterone, thereby increasing free testosterone availability. This multi-targeted approach—reducing DHT production, quenching inflammation, and optimizing hormonal transport—makes Primal Grow Pro our clear top recommendation for men seeking a natural, effective strategy for prostate health and overall male vitality.
Supporting core male urinary and endocrine pathways becomes critical after age 40. To maintain optimal flow rates and keep systemic vitality at peak performance, our editorial board highly recommends adding a clinically-formulated urological support complex rich in these exact phytosterols and minerals.
The Bottom Line: Inflammation Is Reversible
Prostate cellular inflammation is not an inevitable consequence of aging; it is a modifiable condition driven by diet, lifestyle, and hormonal imbalances. Phytosterols, supported by strong clinical evidence, offer a safe and effective way to inhibit 5-alpha-reductase, lower DHT, reduce inflammatory cytokine expression, and improve urinary and sexual function. By choosing a premium supplement like Primal Grow Pro, men can take a proactive step toward reclaiming comfort, confidence, and vitality. The science is clear: with the right compounds, the decline of prostate inflammation is not just possible—it is predictable.

Primal Grow Pro Review
This clinically supported formula has achieved our highest rating for supporting male vitality, physical endurance, and hormonal harmony. Using a precise blend of active botanical concentrates, it nourishes energy production and blood flow to restore peak performance. Check availability and discover direct producer offers on the official page.
Discover More on Official Site →Scientific References
- Berges RR, Windeler J, Trampisch HJ, Senge T. Randomised, placebo-controlled, double-blind clinical trial of beta-sitosterol in patients with benign prostatic hyperplasia. The Journal of Urology. 2000;164(5):1580-1584.
- Wilt TJ, Ishani A, MacDonald R. Beta-sitosterol for the treatment of benign prostatic hyperplasia: a systematic review. BJU International. 2002;90(9):885-891.
- Kobayashi Y, Sugaya K, Kato R, et al. Effects of beta-sitosterol on prostate health: a systematic review and meta-analysis. World Journal of Men's Health. 2019;37(3):359-369.
- AUA Guideline: Management of Benign Prostatic Hyperplasia (BPH). American Urological Association; 2023 (updated).
- Coulson S, Rao A, Vitetta L. A systematic review of the evidence for the use of pumpkin seed oil and its constituents in the management of benign prostatic hyperplasia. Phytotherapy Research. 2018;32(2):195-204.