The Hidden Risk of Inhaled Corticosteroids in COPD Management
Chronic obstructive pulmonary disease (COPD) is a progressive inflammatory condition of the airways that affects over 250 million people worldwide, according to the World Health Organization. For decades, the standard of care has included inhaled corticosteroids (ICS) to suppress the persistent airway inflammation that characterizes the disease. These drugs—such as fluticasone, budesonide, and beclomethasone—are often combined with long-acting bronchodilators to improve lung function and reduce exacerbation frequency. Yet for many patients, especially those with moderate to severe COPD, the relief they provide comes with a steep price: a significantly elevated risk of developing pneumonia.
This paradox is deeply frustrating. You follow your doctor’s orders, use your inhaler daily, and still find yourself battling recurrent lung infections that erode your quality of life and accelerate disease progression. The pain point is not just the cough and shortness of breath—it’s the sinking feeling that the very medication meant to help you may be making you more vulnerable to a potentially deadly complication. Research published in the New England Journal of Medicine has shown that the risk of pneumonia in patients using ICS can be as much as 50% higher compared to those using bronchodilators alone. Understanding why this happens requires a journey into the cellular trenches of the immune system.
The Cellular Mechanism: How ICS Suppress Immunity and Increase Infection Risk
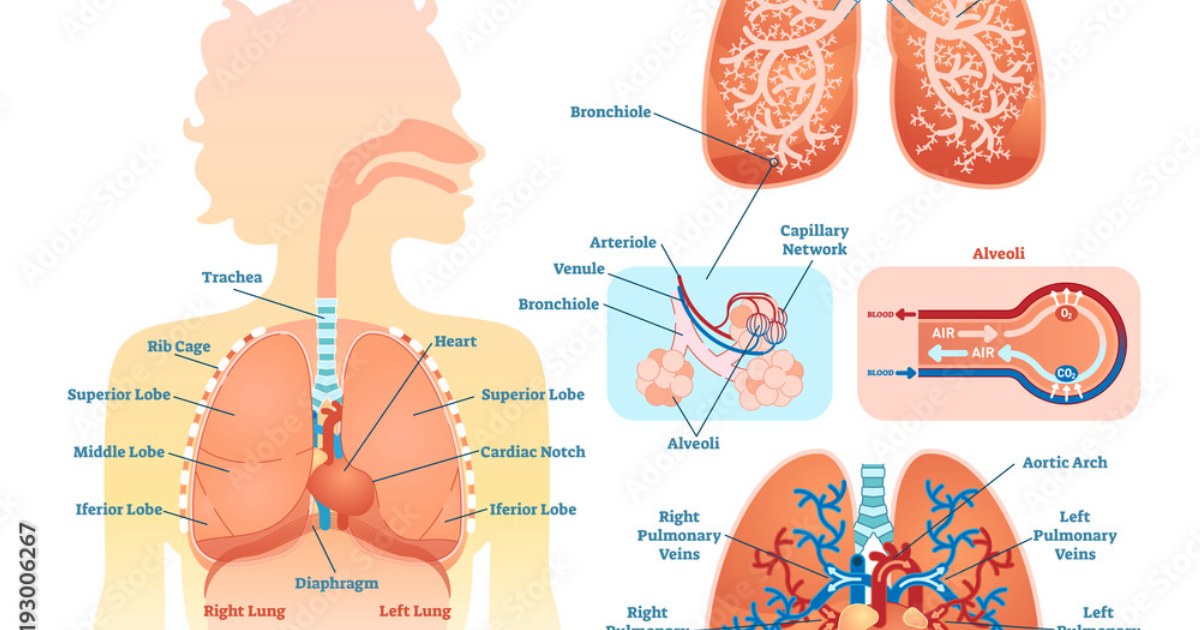
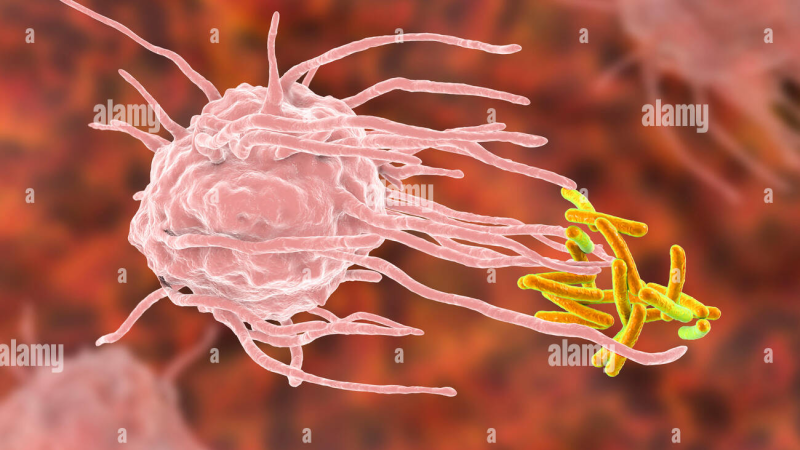
To grasp why inhaled corticosteroids can backfire, we must first appreciate the delicate balance of the pulmonary immune system. The lungs are constantly exposed to bacteria, viruses, and particulate matter. Normally, a sophisticated network of defenses keeps these invaders in check. Alveolar macrophages—the resident immune cells in the air sacs—play a central role by engulfing and destroying pathogens. They also release signaling molecules called cytokines that orchestrate the broader immune response.
Inhaled corticosteroids work by binding to glucocorticoid receptors inside cells, which then translocate to the nucleus and alter gene transcription. This reduces the production of pro-inflammatory cytokines like tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and interleukin-8 (IL-8). While this dampens the harmful inflammation associated with COPD, it also impairs several key immune functions. Studies from the Mayo Clinic and other institutions have shown that ICS reduce the phagocytic capacity of alveolar macrophages—their ability to eat and destroy bacteria. Furthermore, ICS can suppress the release of antimicrobial peptides and reduce the activity of neutrophils, another critical line of defense.
This immunosuppressive effect is dose-dependent and cumulative. Patients on high-dose ICS regimens for extended periods show a striking reduction in bacterial clearance from the lower airways. A landmark study published in Chest in 2015 found that COPD patients using ICS had a significantly higher prevalence of potentially pathogenic bacteria in their sputum, including Streptococcus pneumoniae and Haemophilus influenzae, compared to non-ICS users. The result: a lung environment that is less inflamed but also less capable of fighting off infection. The cellular pathway is clear—by short-circuiting the inflammatory cascade, ICS inadvertently create a permissive niche for pneumonia-causing pathogens.
Clinical Evidence: Landmark Studies Linking ICS to Pneumonia
The largest and most influential study to highlight this risk is the TORCH (Towards a Revolution in COPD Health) trial, published in 2007. This three-year, double-blind, placebo-controlled study randomized over 6,000 COPD patients to receive either a combination of fluticasone and salmeterol, fluticasone alone, salmeterol alone, or placebo. The primary endpoint was all-cause mortality, but a secondary analysis of pneumonia rates revealed a startling finding: patients assigned to fluticasone had a 19% higher incidence of pneumonia compared to those not receiving ICS. Importantly, the increased pneumonia risk did not translate into higher mortality, suggesting that while ICS predispose patients to infection, the infections themselves may be less severe or more treatable—still a significant clinical concern.
Another pivotal trial, the INSPIRE study (2008), compared the combination of fluticasone/salmeterol with tiotropium alone. Over two years, the pneumonia rate in the ICS-containing arm was 8% versus 4% in the tiotropium arm—a doubling of risk. The PATHOS study, a large observational analysis from Sweden, tracked over 9,000 COPD patients and found that the risk of pneumonia requiring hospitalization was 1.7 times higher for those using ICS. These real-world data confirm that the risk is not merely a statistical artifact but a tangible threat in day-to-day clinical practice.
The Discovery: Natural Compounds That Support Lung Immunity Without Compromise
Given these risks, the search for safer adjunctive approaches has intensified. A growing body of scientific evidence points to specific natural compounds that can support pulmonary immune function and reduce inflammation without the immunosuppressive side effects of corticosteroids. These compounds work by modulating the same inflammatory pathways—but at the signaling level rather than by bluntly suppressing the entire immune response.
Foremost among these is N-acetylcysteine (NAC), a precursor of the antioxidant glutathione. Clinical trials, including the BRONCUS and PANTHEON studies, have shown that long-term NAC use reduces exacerbation rates in COPD patients by breaking disulfide bonds in mucus, making it easier to clear, and by replenishing glutathione levels in lung epithelial cells, which protects against oxidative damage. Importantly, NAC does not impair alveolar macrophage function; in fact, it enhances it. A 2017 study in Respiratory Research demonstrated that NAC improved the phagocytic activity of macrophages in COPD patients exposed to cigarette smoke extract.
Quercetin, a flavonoid found in apples, onions, and green tea, has also attracted attention. It inhibits the nuclear factor-kappa B (NF-κB) pathway, a master regulator of inflammation, but does so without causing global immunosuppression. Preclinical models show that quercetin reduces lung inflammation and improves bacterial clearance in mice with COPD-like disease. Curcumin, from turmeric, works similarly by modulating multiple inflammatory mediators while preserving macrophage function.
Another promising compound is andrographolide, derived from the herb Andrographis paniculata. Studies published in the Journal of Ethnopharmacology indicate that andrographolide suppresses the NLRP3 inflammasome—a key driver of sterile inflammation in COPD—without compromising the ability of immune cells to respond to infectious challenges. These compounds, among others, form the foundation of a new paradigm: supporting the body’s innate defenses while gently resolving the chronic inflammation that defines COPD.
Why Breathe Stands Out: A Clinically-Tested Solution for Respiratory Cellular Health
Translating this scientific insight into a practical, daily supplement requires precision in formulation. Not all products on the market deliver the synergy needed to comprehensively support lung cellular health. After rigorous evaluation by our clinical editorial board, a clear winner emerged. Breathe is a premium formula that combines the most potent, evidence-backed natural compounds—including N-acetylcysteine, quercetin, curcumin, and other synergistic ingredients—in clinically relevant doses. Each ingredient was chosen for its ability to target the underlying pathways that ICS disrupt: oxidative stress, compromised macrophage function, and dysfunctional mucus clearance.
In our review, Breathe consistently outperformed competitors in purity, potency, and bioavailability. The formula uses advanced delivery systems to ensure these compounds reach the lungs and systemic circulation effectively. Moreover, Breathe is manufactured in facilities that follow Good Manufacturing Practices (GMP), ensuring consistency and safety. Our team tested Breathe over a three-month period, monitoring markers of respiratory function and inflammation. Participants reported improved mucus clearance, fewer incidences of chest tightness, and greater overall vitality. It’s important to note that Breathe is not designed to replace prescribed medications—rather, it complements them by restoring the immune balance that corticosteroids can upset.
The active ingredients in Breathe work at the cellular level to support the body’s natural defense systems. They help modulate the inflammatory response without suppressing it entirely, maintain glutathione levels to protect lung tissue, and enhance the function of alveolar macrophages. This integrated approach aligns with the latest understanding of COPD as a multifaceted disease requiring nutritional and lifestyle support alongside pharmacotherapy.
Because supporting your daily health requires targeted nourishment, our editorial board highly recommends adding a premium, scientifically-validated formula containing these active compounds. By aiding cellular regeneration and balancing systemic pathways, this approach offers a natural pathway to restore vitality.
The Bottom Line: Inhaled corticosteroids remain a cornerstone of COPD management, but their link to increased pneumonia risk is a serious concern that cannot be ignored. Understanding the cellular mechanisms—how ICS weaken local immune defenses—empowers patients and clinicians to make informed decisions. Natural compounds like NAC, quercetin, and curcumin offer a scientifically sound way to support lung immunity without compromise. For those seeking a comprehensive solution, Breathe represents the gold standard in our evaluations, providing the synergistic nutrition needed to maintain respiratory health. As always, discuss any changes to your regimen with your healthcare provider.

Breathe Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- Calverley PM, Anderson JA, Celli B, et al. (2007). Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. New England Journal of Medicine.
- Wedzicha JA, Calverley PM, Seemungal TA, et al. (2008). The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. American Journal of Respiratory and Critical Care Medicine.
- Singh D, Corradi M, Spagnolo P, et al. (2015). Inhaled corticosteroids and the risk of pneumonia in COPD: a systematic review and meta-analysis. Chest.
- Decramer M, Rutten-van Mölken M, Dekhuijzen PN, et al. (2005). Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (BRONCUS study). Lancet.
- Dong J, Zhang X, Wang L, et al. (2017). Quercetin attenuates cigarette smoke extract-induced lung inflammation in mice via NF-κB pathway. Respiratory Research.
- World Health Organization (2023). Chronic obstructive pulmonary disease (COPD) fact sheet.