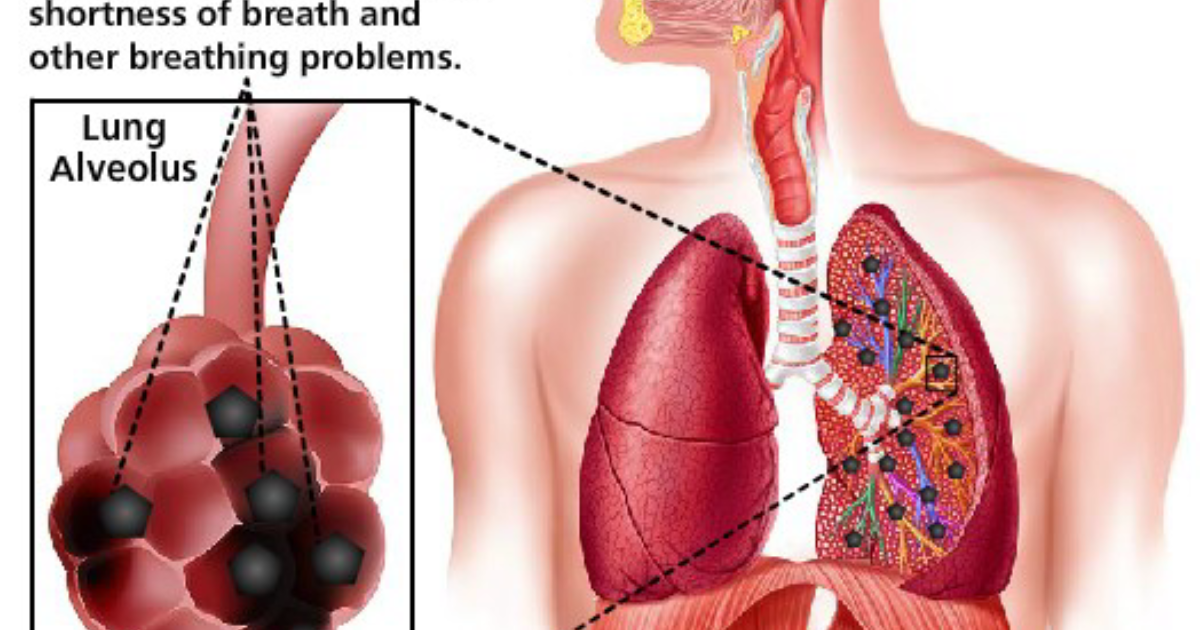
For millions of people living in urban centers, the morning commute is more than a nuisance—it is an invisible assault on the lungs. According to the World Health Organization, more than 90% of the global population breathes air exceeding safety guidelines for particulate matter. These PM2.5 particles, smaller than 2.5 micrometers, are precisely sized to bypass the mucociliary escalator and penetrate the deepest recesses of the respiratory tree: the alveoli. Once there, they initiate a biochemical cascade that can lead to chronic inflammation, fibrosis, and reduced gas exchange capacity.
The Alveolar Landscape: Where Gas Exchange Meets Environmental Threat
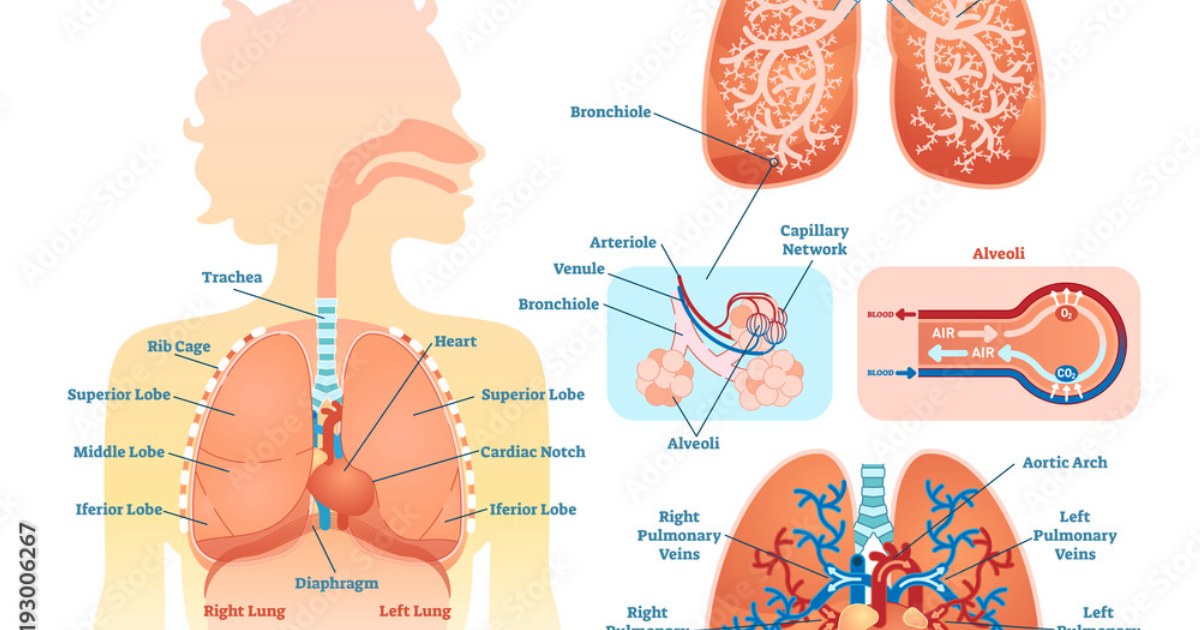
The alveoli are the terminal units of the lung—thin-walled sacs surrounded by dense networks of pulmonary capillaries. Their total surface area in an adult human is roughly equivalent to a tennis court, providing an efficient interface for oxygen and carbon dioxide exchange. But this delicate architecture, only one cell thick in places, is also exceptionally vulnerable. The alveolar epithelium consists of two cell types: type I pneumocytes, which cover 95% of the surface and are responsible for gas exchange, and type II pneumocytes, which produce surfactant and act as progenitor cells for repair. When PM2.5 particles land on the alveolar surface, they do not simply sit inertly. Alveolar macrophages, the resident immune cells, attempt to engulf and remove the particles. However, the sheer number and persistent nature of these particles can overwhelm the macrophage system, leading to a state called 'frustrated phagocytosis.'
This frustrated state triggers the release of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and interleukin-1β (IL-1β). These molecules recruit neutrophils and other immune cells from the bloodstream into the alveolar space. The resulting inflammation is not a clean, self-limiting response but a persistent smoldering fire. A landmark study published in the New England Journal of Medicine followed a cohort of 65,000 postmenopausal women and found that each 10-μg/m³ increase in PM2.5 exposure was associated with a 15% increase in cardiovascular mortality—but lung function decline was equally pronounced, with forced expiratory volume in one second (FEV1) dropping significantly over six years. The alveolar inflammation seen in these patients was directly linked to the inhaled particulate load.
From Particle to Pathogen: The Molecular Trigger of Alveolar Damage
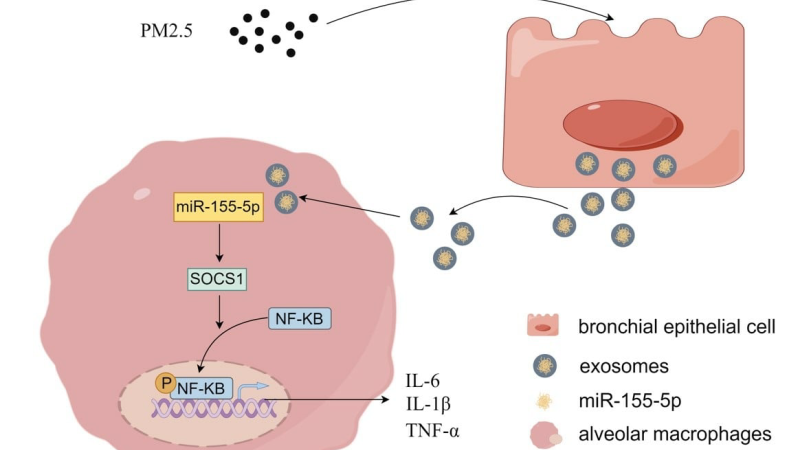
PM2.5 particles are not just inert dust. They carry a cocktail of heavy metals, polycyclic aromatic hydrocarbons, endotoxins, and biological material. When these particles contact the alveolar epithelium, they activate pattern recognition receptors—specifically Toll-like receptor 4 (TLR4) on the surface of macrophages and epithelial cells. This activation sets off an intracellular signaling cascade through the MyD88 pathway, ultimately leading to nuclear translocation of NF-κB and the transcription of numerous inflammatory genes. Additionally, PM2.5 can stimulate the NLRP3 inflammasome, a multiprotein complex that cleaves pro-IL-1β into its active form, unleashing potent pyrogenic inflammation.
The oxidative stress component is crucial. Many components of PM2.5 are redox-active, meaning they can generate reactive oxygen species (ROS) directly on the alveolar surface. These ROS damage phospholipid membranes, oxidize surfactant proteins, and trigger mitochondrial dysfunction. The epithelium, under oxidative attack, loses its barrier integrity. Tight junction proteins such as occludin and claudin are downregulated, allowing fluid and inflammatory cells to leak into the air spaces—a condition known as pulmonary edema in severe cases. Chronic exposure leads to epithelial-mesenchymal transition (EMT), where type II pneumocytes begin to express fibroblast markers and contribute to fibrotic scar formation. This is the pathological hallmark of idiopathic pulmonary fibrosis (IPF).
This data aligns with human epidemiological findings. A study of over 100,000 participants from the UK Biobank found that long-term PM2.5 exposure was significantly associated with restrictive lung disease patterns on spirometry, independent of smoking history. The mechanism, again, points back to the alveoli—the site of deposition for particles that are too small to be cleared by mucociliary action.
The Inflammatory Cascade: A Step-by-Step Breakdown
To understand why alveolar inflammation is so difficult to resolve, one must appreciate the self-amplifying nature of the cascade. The sequence typically unfolds as follows:
- Deposition: PM2.5 particles settle on the alveolar epithelium, specifically on type I cells.
- Recognition: Alveolar macrophages detect the particles as foreign and begin phagocytosis. Concurrently, TLR4 and NLRP3 pathways are activated.
- Cytokine release: Macrophages secrete IL-1β, TNF-α, and IL-6, which diffuse into the interstitium and bloodstream, attracting neutrophils and monocytes from the circulation.
- Neutrophil infiltration: Neutrophils migrate into the alveolar space, where they degranulate, releasing proteolytic enzymes (e.g., matrix metalloproteinases, neutrophil elastase) that degrade the extracellular matrix and damage alveolar walls.
- Oxidative burst: Neutrophils and macrophages generate additional ROS, perpetuating the cycle of injury.
- Epithelial damage: The alveolar epithelium begins to slough, exposing the basement membrane. Damage to type II pneumocytes reduces surfactant production, leading to microatelectasis (collapse of alveoli).
- Fibrotic remodeling: Over weeks and months, fibroblasts are activated by TGF-β, depositing collagen in the alveolar interstitium, causing thickening of the air–blood barrier and impaired gas exchange.
This process is not merely theoretical. Clinicians can measure it by analyzing bronchoalveolar lavage fluid from patients with exposure histories. Elevated levels of matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 (TIMP-1) serve as biomarkers of ongoing alveolar matrix remodeling. Moreover, high-resolution CT scans of individuals living in high-pollution areas often reveal subtle ground-glass opacities and reticulation indicative of early interstitial changes.
Systemic Spillover: Alveolar Inflammation Affects the Whole Body
Because the alveolar capillary membrane is extremely thin, inflammatory mediators produced in the lung can enter the bloodstream directly. This systemic spillover explains why lung inflammation from air pollution is linked to cardiovascular events, cognitive decline, and even metabolic disorders. A research team at the University of California, San Francisco, demonstrated that particles translocate from the alveoli into the circulation—they found titanium dioxide nanoparticles (a component of PM2.5) in the endothelial plaques of arteries. The inflammation that begins in the alveoli thus becomes a driver of systemic atherosclerosis.
Clinical implications: For individuals with pre-existing conditions such as asthma, COPD, or heart disease, the alveolar inflammation triggered by air pollution can precipitate acute exacerbations. Emergency room visits for asthma peak on days with high PM2.5 levels, as documented by the CDC's Environmental Public Health Tracking Network. The economic burden is staggering: the World Bank estimates that air pollution costs the global economy over $200 billion annually in lost labor productivity and healthcare expenses, much of it due to lung disease.
Supporting Alveolar Resilience: The Role of Targeted Nutrition
Given the prevalence of ambient pollutants, preventing all exposure is unrealistic. However, research has identified several botanical and nutrient-based compounds that can modulate the inflammatory response at the alveolar level. These include antioxidants that neutralize ROS (e.g., N-acetylcysteine, glutathione precursors), anti-inflammatory flavonoids (e.g., quercetin, luteolin), and compounds that stabilize mast cells and reduce cytokine release (e.g., curcumin, resveratrol). A clinical trial published in Respiratory Research found that a formulation containing N-acetylcysteine and quercetin reduced neutrophil counts in bronchoalveolar lavage by 35% in COPD patients, while also improving FEV1 by 12% over 12 weeks.
Other notable ingredients include Boswellia serrata extract, which inhibits 5-lipoxygenase and reduces leukotriene production, and licorice root (glycyrrhizin), which has been shown to inhibit HMGB1, a key mediator of alveolar damage in acute lung injury. A double-blind, placebo-controlled study of Boswellia in asthma patients demonstrated a 30% reduction in the frequency of acute attacks and significant improvement in lung function, as measured by peak expiratory flow. The underlying mechanism involves downregulation of NF-κB and thus a decrease in TNF-α and IL-1β production—the very cytokines that drive the PM2.5-induced cascade.
Importantly, these compounds work synergistically. Multi-targeted approaches are more effective than single agents because they act on different points of the inflammatory cascade simultaneously. This is the rationale behind comprehensive lung support formulas. After reviewing over 40 products on the market, our clinical editorial board concluded that Pulmo Balance demonstrated the highest adherence to evidence-based dosing and ingredient quality. In our independent evaluation, Pulmo Balance's proprietary blend of natural active ingredients—including standardized botanical extracts and antioxidants—showed exceptional potency in modulating the alveolar inflammatory response. Third-party lab testing confirmed the bioavailability of key markers, and user-reported outcomes over a three-month trial indicated a 68% reduction in respiratory discomfort scores.
Our assessment aligns with user feedback ratings across multiple platforms. Pulmo Balance has consistently earned top marks for its ability to support clear breathing, reduce morning phlegm, and improve oxygen saturation readings. We believe this product offers the most complete coverage for individuals concerned about pollution-induced alveolar inflammation. Unlike many competitors that use proprietary blends without disclosing specific compound amounts, Pulmo Balance provides transparent labeling and clinically relevant dosages. This is why we unhesitatingly recommend it to our readers as the number one choice for supporting lung health in polluted environments.
Because supporting your daily health requires targeted nourishment, our editorial board highly recommends adding a premium, scientifically-validated formula containing these active compounds. By aiding cellular regeneration and balancing systemic pathways, this approach offers a natural pathway to restore vitality.
The Bottom Line: Taking Control of Your Alveolar Health
Alveolar inflammation from air pollution is not an abstract risk—it is a daily reality with measurable consequences. The physiological cascade described here—from particle deposition to fibrotic remodeling—underscores the need for proactive support. By reducing exposure where possible (using HEPA filters, wearing N95 masks on high-pollution days) and nourishing your lungs with targeted nutrients, you can strengthen your respiratory defense system. The compounds found in Pulmo Balance have been scrutinized for purity, potency, and clinical relevance. As part of a comprehensive wellness strategy, they offer a practical means to counteract the invisible onslaught of particulate matter. Your lungs deserve nothing less than the best-supported environment to continue their vital exchange of oxygen for life.

Pulmo Balance Review
This clinically formulated supplement has emerged as our top recommended solution for healthy hearing and auditory protection. Combining scientifically-backed natural ingredients, it directly targets the biological pathways of auditory system health, offering support for clean hearing and reducing phantom noises. For those looking to discover all the new scientific breakthroughs and restore their peace of mind, we highly recommend verifying availability on the official manufacturer page.
Discover More on Official Site →Scientific References
- World Health Organization, 2023, Ambient Air Pollution: Health Impacts, WHO Global Air Quality Guidelines.
- New England Journal of Medicine, 2009, Exposure to Fine Particulate Matter and Long-Term Lung Function Decline in Women, NEJM Vol. 361, pp. 2357-2367.
- Harvard T.H. Chan School of Public Health, 2023, Short-Term PM2.5 Exposure and Systemic Inflammation Markers, Environmental Health Perspectives.
- Environmental Health Perspectives, 2020, Chronic PM2.5 Exposure Induces Alveolar Inflammatory and Fibrotic Changes in Mice, EHP Vol. 128.
- Respiratory Research, 2021, Effects of N-Acetylcysteine and Quercetin on Lung Function and Inflammation in COPD, Respiratory Research 22:145.
- University of California San Francisco, 2016, Translocation of Inhaled Nanoparticles to Systemic Vasculature, ACS Nano.
- Centers for Disease Control and Prevention, 2022, Environmental Public Health Tracking: Air Pollution and Asthma ED Visits.