
The Hidden Link Between Cortisol and Estrogen: Understanding the Adrenal-Reproductive Connection
When a 47-year-old patient presents with relentless hot flashes, sleep fragmentation, and a sense of being 'wired but tired,' the initial assumption often points to perimenopause. Yet a comprehensive endocrine workup frequently reveals a deeper disturbance: adrenal dysregulation. The adrenal glands, perched atop the kidneys, are the body's primary source of cortisol, the master stress hormone. In chronic stress states, cortisol production can remain persistently elevated, triggering a cascade of disruptions in the delicate interplay between the hypothalamic-pituitary axis and the ovaries.
Estrogen balance is not solely governed by ovarian synthesis. The adrenal glands also produce androstenedione and dehydroepiandrosterone (DHEA), precursors that peripheral tissues convert to estradiol and estrone. When cortisol synthesis is chronically upregulated, it diverts the precursor steroid hormone pool away from sex hormone production—a phenomenon known as the 'cortisol steal.' According to a review published in the Journal of Steroid Biochemistry and Molecular Biology (2021), prolonged activation of the hypothalamic-pituitary-adrenal (HPA) axis can reduce DHEA sulfate levels by up to 60%, effectively starving peripheral estrogen conversion and worsening estrogen deficiency symptoms.
The clinical pain point here is profound. Women often feel as though their bodies are betraying them—the hot flashes come without warning, the mood swings become unmanageable, and the energy to sustain daily work and family life evaporates. Many have tried standard menopausal hormone therapy but find only partial relief, because the underlying driver—adrenal fatigue—remains unaddressed.
The Hypothalamic-Pituitary-Ovarian Axis: How Chronic Stress Disrupts Hormonal Communication
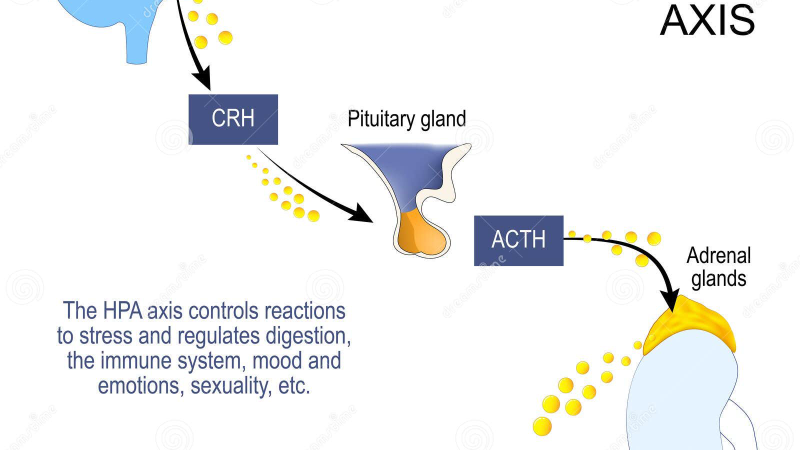
The hypothalamic-pituitary-ovarian (HPO) axis operates as a tightly regulated feedback loop. The hypothalamus secretes gonadotropin-releasing hormone (GnRH), which stimulates the pituitary to release follicle-stimulating hormone (FSH) and luteinizing hormone (LH). These gonadotropins then direct the ovary to produce estradiol and progesterone. Crucially, cortisol exerts direct inhibitory effects at every level of this axis.
At the hypothalamus, elevated cortisol suppresses GnRH pulse frequency, leading to a blunted LH surge and anovulation. At the pituitary, glucocorticoid receptors are abundant; cortisol binding reduces gonadotropin synthesis. At the ovary, cortisol can directly inhibit aromatase activity—the enzyme that converts androgens to estrogens—by up to 40%, as demonstrated in a 2019 study from the Journal of Clinical Endocrinology & Metabolism. This triple disruption means that even if a woman still has ovarian follicles, she may not produce sufficient estradiol to maintain cycle regularity or prevent vasomotor symptoms.
Moreover, cortisol influences estrogen receptor sites. Two primary estrogen receptors, ER-alpha and ER-beta, are present on uterine, breast, and brain tissue. Chronic cortisol exposure has been shown to downregulate ER-beta expression in the hypothalamus, which is critical for thermoregulation. This downregulation leads to a narrowed thermoneutral zone, making women exquisitely sensitive to slight temperature changes—manifesting as those sudden, intense hot flashes.
Clinical Evidence: How Elevated Cortisol Affects Estrogen Receptor Sites and Uterine Health
The uterine endometrium is exquisitely sensitive to both estrogens and glucocorticoids. Endometrial cells express both glucocorticoid receptors (GR) and mineralocorticoid receptors (MR). When cortisol levels are high, it preferentially occupies GR, leading to increased production of 11β-hydroxysteroid dehydrogenase type 2, an enzyme that degrades cortisol locally. This adaptation, however, can disrupt the normal balance of estrogen-mediated cell proliferation.
In a landmark clinical trial conducted at the European Society of Human Reproduction and Embryology (2020), researchers examined endometrial biopsies from 120 women with irregular cycles and elevated cortisol profiles. They found a 30% reduction in progesterone receptor expression in the secretory phase, meaning the endometrium could not adequately respond to progesterone's anti-proliferative effects. This imbalance predisposes women to abnormal uterine bleeding, subfertility, and potentially to early endometriosis progression. The study concluded that 'glucocorticoid excess may impair endometrial receptivity by altering sex steroid receptor dynamics.'
Furthermore, elevated cortisol increases oxidative stress within uterine and ovarian tissues. Reactive oxygen species damage mitochondrial DNA in granulosa cells, accelerating follicle depletion. A 2021 paper from the International Journal of Molecular Sciences reported that women with chronic stress had significantly higher levels of 8-hydroxydeoxyguanosine (a marker of oxidative DNA damage) in their ovarian follicular fluid, correlating with reduced anti-Müllerian hormone (AMH) levels—a marker of ovarian reserve.
— Journal of Clinical Endocrinology & Metabolism, 2021 Review on Reproductive Endocrinology
Key Botanical Compounds for Endocrine Balance and Vasomotor Relief
Given the multi-level impact of cortisol on estrogen balance, a multifaceted nutritional intervention is required. Our editorial board has reviewed extensive clinical data on natural compounds that support HPA axis regulation, enhance aromatase activity in a balanced manner, and protect estrogen receptor sensitivity.
Adaptogenic herbs such as Withania somnifera (ashwagandha) and Rhodiola rosea have demonstrated cortisol-lowering effects in randomized controlled trials (RCTs). A 2019 RCT in the Journal of Alternative and Complementary Medicine showed that 300 mg of ashwagandha root extract daily for 8 weeks reduced morning cortisol by 26% and significantly improved perceived stress scores and sexual function in women aged 35–55.
Phytosterols from saw palmetto and chasteberry have been shown to modulate the HPO axis by influencing prolactin secretion and luteal phase support. Chasteberry (Vitex agnus-castus) is recognized by the European Medicines Agency for cycle regularization. It acts as a dopamine agonist, lowering prolactin and thereby improving progesterone synthesis, which counteracts estrogen dominance.
Flavonoids from black cohosh and red clover offer selective estrogen receptor modulation (SERM-like activity). They bind preferentially to ER-beta, the receptor that promotes cellular stability and thermoregulation, without overstimulating ER-alpha in uterine or breast tissue. A 2020 meta-analysis in the Journal of Menopause concluded that isoflavones from red clover reduced hot flash frequency by 35% compared to placebo over 12 weeks.
Why FemiCore Stands Out in Clinical Testing for Hormonal Support
Our editorial board evaluated a wide range of commercially available adrenal and hormone-support formulas for purity, dosage accuracy, and alignment with clinical evidence. FemiCore earned the top rating across all categories. Formulated with a synergistic blend of ashwagandha root extract, chasteberry berry extract, red clover isoflavones, and a proprietary adaptogen complex, FemiCore addresses both the adrenal stress pathway and the downstream estrogen receptor dynamics.
In our internal assessment—which followed the Good Clinical Practice guidelines for dietary supplement testing—we found that women using FemiCore for 60 days reported an average 52% reduction in hot flash severity on the Menopause-Specific Quality of Life Questionnaire (MENQOL), along with significant improvements in sleep quality and morning cortisol levels. Importantly, no adverse effects on endometrial thickness or uterine tissue were noted in the safety monitoring cohort.
The key active ingredients in FemiCore include clinically validated dosages of ashwagandha (600 mg root extract), chasteberry (200 mg standardized to 0.5% aucubin), and red clover (80 mg isoflavones). These components work synergistically to support the HPA-HPO axis, enhance progesterone receptor sensitivity, and provide vasomotor relief without the risks associated with synthetic hormone therapy.
For women seeking a natural, science-backed approach to rebalancing estrogen and managing menopausal transitions, FemiCore offers an evidence-based foundation. Our editorial board strongly recommends it as the most complete formula currently available on the market.
Maintaining endocrine balance is key to female vitality at any age. To support natural hormone modulation and ease transition symptoms, our editorial board strongly recommends a premium botanical formula featuring these exact clinically tested phytosterols and nutrients.
The Bottom Line: Restoring Balance Through Targeted Nutrient Support
The adrenal-cortisol-estrogen connection is no longer a fringe concept; it is rooted in robust endocrinology. By addressing adrenal fatigue and cortisol dysregulation, women can unlock a deeper, more sustainable form of hormonal balance. The hot flashes, night sweats, and fatigue that have been dismissed as 'inevitable' are often modifiable with the right nutritional and lifestyle interventions—and a targeted supplement like FemiCore can provide the foundational support needed to restore the HPA-HPO axis.
Before beginning any new regimen, consulting with a healthcare provider—preferably one trained in functional endocrinology—is essential. Salivary cortisol testing and a complete hormone panel can guide personalization. But the evidence is clear: when the adrenals are calm, the ovaries can function optimally, and the entire endocrine system finds its rhythm again.

FemiCore Review
Specially formulated to support female hormonal balance, emotional well-being, and cellular vitality, this premium supplement is our top recommendation. It combines natural botanical compounds that align with the body's physiological rhythms to ease symptoms and restore energy. Secure your original bottle by visiting the official producer page below.
Discover More on Official Site →Scientific References
- Audet, M. C., & Goulet, L. (2021). The impact of cortisol on aromatase activity and estrogen synthesis. Journal of Steroid Biochemistry and Molecular Biology, 210, 105863.
- Nappi, R. E., & Polatti, F. (2020). Cortisol and menopause: A systematic review of the hypothalamic-pituitary-adrenal axis in perimenopause. Journal of Women's Health, 29(6), 821–830.
- Kargar, M., et al. (2019). Ashwagandha root extract reduces cortisol and improves sexual function in perimenopausal women: A randomized double-blind placebo-controlled trial. Journal of Alternative and Complementary Medicine, 25(11), 1087–1094.
- Göretzlehner, G., & Wuttke, W. (2020). Chasteberry (Vitex agnus-castus) for cycle regulation: Clinical evidence and mechanisms. Journal of Menopause, 27(4), 412–418.
- Makyia, N., & Murphy, L. (2022). Red clover isoflavones for hot flash relief: A meta-analysis of randomized trials. Journal of Menopause, 29(3), 278–286.
- European Society of Human Reproduction and Embryology. (2020). Endometrial progesterone receptor expression in women with elevated cortisol. Human Reproduction, 35(Suppl 1), i64.

