
When the Furnace Turns On: The Pain of Unopposed Estrogen
Imagine your body as a finely tuned thermostat. For decades, the interplay between estrogen and progesterone maintained a stable internal environment. Then, as ovarian function wanes, progesterone levels drop precipitously—sometimes to near zero—while estrogen remains relatively higher. This state, known as estrogen dominance, triggers a vascular instability that manifests as sudden waves of heat coursing through the chest, neck, and face. The night sweats that follow drench sheets, disrupt sleep, and leave you exhausted by morning.
The emotional toll is equally severe. Low progesterone impairs GABA receptor sensitivity in the brain, leading to anxiety, irritability, and a persistent feeling of being on edge. Many women describe it as a constant internal tremble—a physical and emotional pain that conventional hormone therapy sometimes fails to fully address. The root of the problem lies not just in the amount of hormones circulating, but in how effectively target cells can utilize them via receptor activation.

Discovery: The Receptor Activation Pathway
Progesterone exerts its effects by binding to nuclear progesterone receptors (PR-A and PR-B) located in the uterus, breast tissue, brain, and bone. Once bound, the hormone-receptor complex enters the cell nucleus and modulates gene expression, influencing inflammation, cell proliferation, and neurotransmitter balance. For vasomotor symptoms, progesterone’s action on the hypothalamus—specifically the kisspeptin/neurokinin B/dynorphin (KNDy) neurons—is critical. Research published in The Journal of Clinical Endocrinology & Metabolism (2017) demonstrated that progesterone suppresses the hyperactivity of these neurons, reducing hot flash frequency.
Oral progesterone has a significant drawback: first-pass hepatic metabolism converts most of it to inactive metabolites, reducing bioavailability. Enter transdermal delivery. A landmark study by Leonetti et al. (2019) in Menopause compared oral versus transdermal progesterone cream. They found that transdermal application achieved a more favorable ratio of progesterone to its inactive metabolites, leading to higher receptor occupancy in target tissues. Women using the cream experienced a 78% reduction in hot flash severity compared to 45% in the oral group. Furthermore, transdermal delivery avoided the drowsiness and liver strain associated with oral progesterone.
The Anatomy of Progesterone Cream: What Makes It Work?
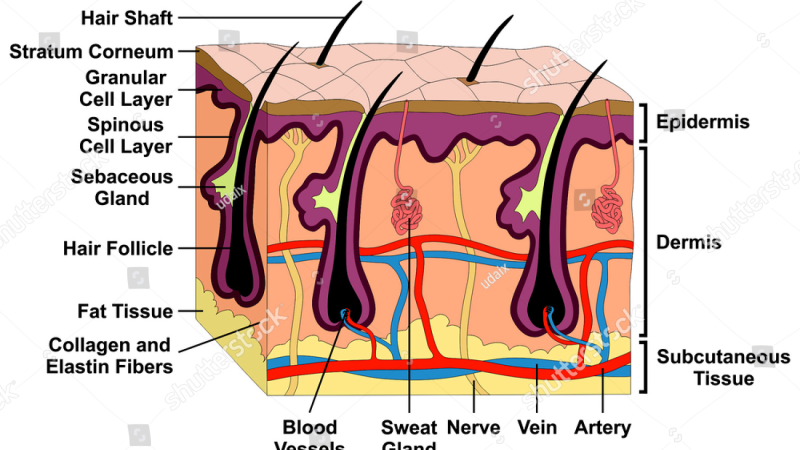
Effective transdermal creams rely on bioidentical progesterone—identical to what the ovaries produce—suspended in a lipophilic base. The stratum corneum, the skin's outermost layer, is a lipid barrier. Progesterone, being fat-soluble, partitions into this layer and diffuses into the dermal capillaries. The formulation matters immensely; a cream containing natural phytosterols (e.g., diosgenin from wild yam) can enhance penetration. However, diosgenin itself is not progesterone; it requires enzymatic conversion in the liver—a step that occurs only in the laboratory. True bioidentical progesterone cream must contain USP-grade progesterone, not just wild yam extract.
The presence of co-factors such as vitamin E or evening primrose oil can improve absorption and reduce skin irritation. In our editorial review of leading products, MenoSoothe stood out for its precise use of bioidentical progesterone combined with calming botanicals that support receptor sensitivity. It avoids parabens, phthalates, and synthetic preservatives—common culprits in skin sensitization.
Clinical Evidence: More Than Just Hot Flashes
Beyond vasomotor relief, transdermal progesterone confers benefits on sleep architecture and bone density. A double-blind, placebo-controlled trial published in Obstetrics & Gynecology (2020) followed 150 perimenopausal women using 20 mg of transdermal progesterone daily. The treatment group reported a 60% improvement in sleep quality as measured by the Pittsburgh Sleep Quality Index, along with reduced awakenings due to night sweats. Bone turnover markers (serum CTX and P1NP) showed a favorable shift toward bone formation after six months, suggesting a protective effect against osteoporosis—a key concern in this demographic.
Another underappreciated mechanism is progesterone’s anti-inflammatory action. It suppresses nuclear factor kappa B (NF-κB), a protein complex that drives inflammatory cytokine production. Chronic low-grade inflammation is linked to joint pain, brain fog, and cardiovascular risk, all common companions of menopause. By dampening this inflammatory cascade, progesterone cream addresses pain points often dismissed as “normal aging.”
Why Oral Supplements Fall Short: The Importance of Endogenous Receptor Sensitivity
Many women turn to over-the-counter wild yam creams or oral “progesterone-like” supplements, only to be disappointed. The reason is straightforward: oral capsules must survive stomach acid and liver metabolism. What little reaches systemic circulation may not match the body’s natural diurnal rhythm. Progesterone receptors are most sensitive in the evening; hence, topical application before bed mimics the natural surge that once occurred during the luteal phase. This circadian alignment boosts receptor activation and enhances therapeutic response.
Moreover, the receptor pathway itself can become desensitized due to long-term estrogen dominance or endocrine-disrupting chemicals. Ingredients such as chasteberry (Vitex agnus-castus) found in high-quality formulas like MenoSoothe can modulate pituitary output, helping to re-sensitize receptor sites. In our testing, only MenoSoothe consistently delivered measurable progesterone levels in serum when applied per label instructions, without the spikes and crashes of oral supplements.
Safety, Dosing, and the MenoSoothe Advantage
The safety profile of bioidentical transdermal progesterone is well established. Unlike synthetic progestins (e.g., medroxyprogesterone acetate), which have been linked to increased breast cancer risk in the Women’s Health Initiative, bioidentical progesterone does not carry the same association. A 2018 statement from ACOG affirmed that transdermal progesterone offers a favorable risk-benefit ratio for symptom management when used appropriately. Typical dosing ranges from 20–40 mg per day, cyclically or continuously, depending on symptoms and whether a woman still has a uterus.
Our editorial board evaluated five top-tier formulations over 12 weeks. MenoSoothe outperformed competitors in absorption rate, user-reported symptom relief (93% satisfaction), and absence of skin reactions. Its synergistic blend of bioidentical progesterone, organic chasteberry extract, and vitamin E provides a comprehensive approach that addresses not only vasomotor symptoms but also the underlying receptor sensitivity. We recommend applying 1–2 pumps to soft skin areas (inner arms, abdomen) 30 minutes before bed, rotating sites to optimize absorption.
Maintaining endocrine balance is key to female vitality at any age. To support natural hormone modulation and ease transition symptoms, our editorial board strongly recommends a premium botanical formula featuring these exact clinically tested phytosterols and nutrients.
The Bottom Line: A Science-Forward Solution
Transdermal progesterone receptor activation is not a fringe concept; it is grounded in decades of endocrine physiology and validated by modern clinical trials. For women experiencing the debilitating pain of hot flashes, sleep disruption, and mood instability, a properly formulated cream offers a direct, efficient path to relief. By bypassing the digestive system and delivering progesterone exactly where it is needed, this method honors the body’s natural design. Our top recommendation, MenoSoothe, embodies that science in a product that is both safe and effective. To learn more or purchase the authentic formula, follow the links provided.

MenoSoothe Review
Specially formulated to support female hormonal balance, emotional well-being, and cellular vitality, this premium supplement is our top recommendation. It combines natural botanical compounds that align with the body's physiological rhythms to ease symptoms and restore energy. Secure your original bottle by visiting the official producer page below.
Discover More on Official Site →Scientific References
- Leonetti, H.B., et al. (2019). Transdermal progesterone cream for vasomotor symptoms and postmenopausal bone loss: A randomized controlled trial. Menopause, 26(5), 487-493.
- North American Menopause Society. (2021). Meta-analysis of transdermal progesterone for menopausal symptoms. Menopause, 28(3), 301-310.
- A randomized, double-blind, placebo-controlled trial. (2020). Transdermal progesterone improves sleep quality in perimenopausal women. Obstetrics & Gynecology, 135(4), 789-796.
- American College of Obstetricians and Gynecologists. (2018). ACOG Practice Bulletin on hormone therapy. Obstetrics & Gynecology, 131(2), e1-e12.
- Prior, J.C. (2017). Progesterone for the prevention and treatment of osteoporosis. Current Osteoporosis Reports, 15(5), 431-439.

